
Executive Summary: The Industrialization of the Soul
The Thesis: Psychotherapy is not “evolving”; it is being dismantled. The convergence of for-profit insurance, administrative bloat in universities, and the fetishization of “manualized” care has stripped the profession of its depth.
The Core Rot:
- The Academic Factory: Universities now view students as “products” to be sold. They have replaced tenure-track professors with adjuncts who teach to the test, producing clinicians who know statistics but cannot sit with suffering.
- The 15-Minute Med Check: The medical model has abandoned the “physician of the soul” in favor of the prescriber, leaving patients medicated but unheard.
- The CBT Monopoly: We teach modalities like CBT not because they are “better,” but because they fit neatly into insurance spreadsheets.
The Result: A two-tier mental health system where deep healing is a luxury good, and the public system is a revolving door of crisis management.
Is the Corporatization of Healthcare and Academia Ruining Psychotherapy?
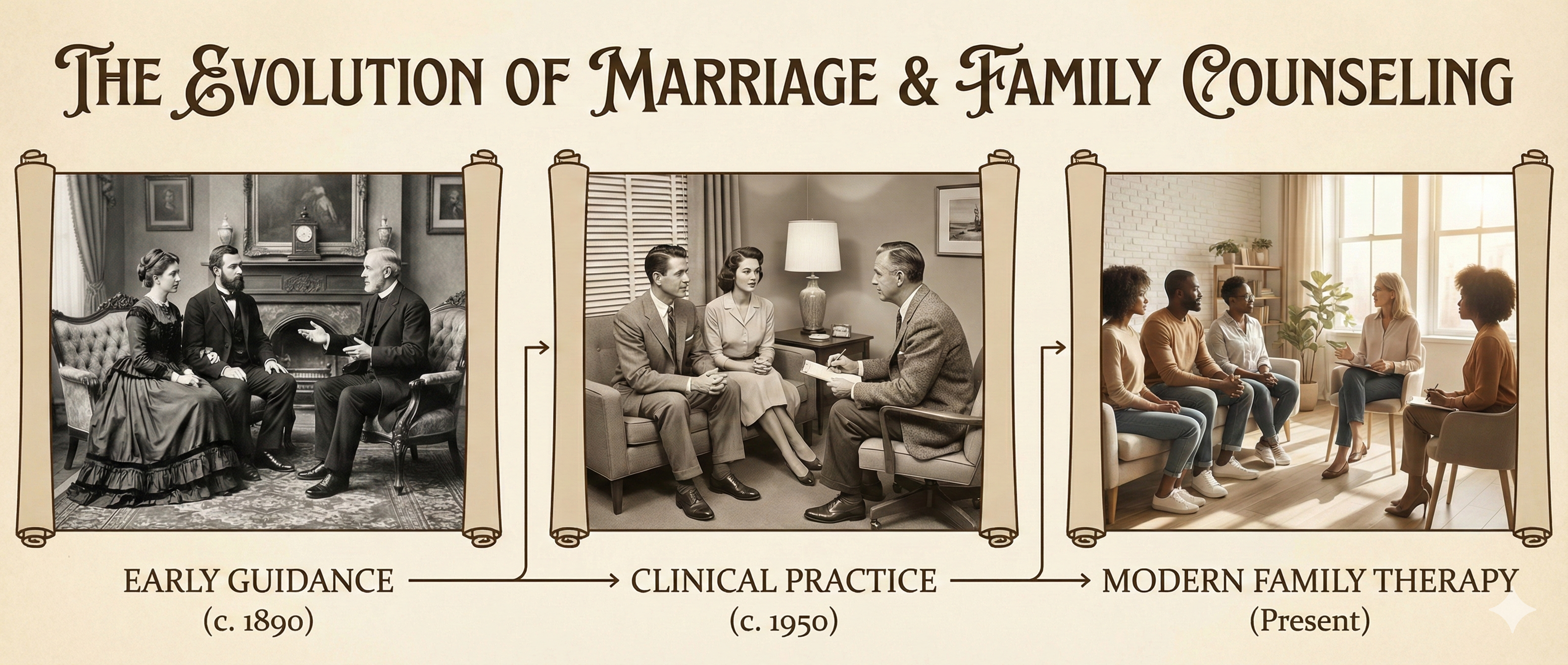
There was a time, not so long ago, when a psychiatrist would spend an entire hour with a patient. They would explore the patient’s history, their dreams, their fears, and the architecture of their relationships. Today, that proposition seems almost mythical, like a story from a bygone era. The standard of care has devolved into the “15-minute med check”—a rapid-fire assessment of symptoms followed by a prescription pad.
This shift is not an accident, and it is not “progress.” It is the result of a decades-long process of Corporatization that has turned mental health from a healing art into an industrial assembly line. We are witnessing the systematic dismantling of depth psychology in favor of “deliverables,” “outcomes,” and “efficiency.”
Part I: The Medical Model vs. The Healing Relationship
I hate to side with patients against my peers in the medical profession, but when a patient tells me, “My doctor didn’t listen; he just wrote a script in five minutes,” they are usually right. Five minutes is not enough time to understand a human being. It is barely enough time to introduce yourself.
We are currently seeing a massive retreat of MDs from the practice of psychotherapy. [cite_start]According to a 2010 study, 89% of psychiatrists solely used drug therapy[cite: 1]. This is a stark increase from 1988, when roughly half of psychiatrists still practiced talk therapy. The “Physician of the Soul” has been replaced by the “Technician of the Synapse.”
The “Treatment Resistant” Myth
Many patients come to us labeled “Treatment Resistant.” In reality, they are often suffering from conditions that cannot be fixed by serotonin reuptake inhibitors. They are dealing with:
* Complex Grief: The loss of a loved one, a career, or an identity.
* Systemic Abuse: Living in a toxic household or workplace that keeps their nervous system in a state of chronic threat.
* Existential Crisis: A loss of meaning, purpose, or connection to the divine.
When we try to drug these problems away without understanding their roots, we are not practicing medicine; we are practicing social control. We are telling the patient that their reasonable reaction to an unreasonable world is a biological error.
Part II: The Decay of the University System
If the doctors aren’t doing therapy, surely the therapists are, right? Unfortunately, the institutions responsible for training our next generation of healers—the universities—have been hollowed out by corporate logic.
[cite_start]
The cost of a public university education has risen by over 3,000% since 1970[cite: 18]. Where is that money going?
It is certainly not going to the professors. Tenure-track positions—the kind that allow professors the freedom to teach complex, controversial, or deep material—have been slashed. [cite_start]They now make up only about a quarter of faculty positions[cite: 19].
Instead, classes are taught by underpaid adjuncts who often have little to no clinical experience. They are teaching from a textbook they may have read for the first time the week before.
Students as “Products”
In the new corporate university, the student is not a student; they are a “customer.” And worse, in board meetings, graduates are referred to as “products” or “deliverables.”
The goal is no longer to produce a wise, capable healer. The goal is to get the “product” off the assembly line as quickly and cheaply as possible. This means:
- Grade Inflation: Because you don’t fail a paying customer.
- Teaching to the Test: Preparing students for licensure exams rather than the messy reality of clinical work.
- Manualized Therapy: Teaching simple, formulaic models like basic CBT because they are easy to grade, rather than complex models like Jungian Analysis or Existential Therapy which require wisdom and intuition.
I often ask recent graduates, “What is the last thing you learned that actually helps you sit with a suffering patient?” The answer is usually a blank stare. They know statistics. They know the DSM-5. But they do not know how to be with someone who is falling apart.
Part III: The “Evidence-Based” Trap
The corporate takeover relies on a specific linguistic weapon: “Evidence-Based Practice.”
It sounds scientific, but in the current landscape, it is often a marketing term for “Cheap and Fast.”
Why CBT Dominates the Academy:
We teach Cognitive Behavioral Therapy (CBT) not necessarily because it is the most effective treatment for deep trauma, but because it is the easiest to measure in a short-term study. It fits the “medical model”—diagnose the symptom, apply the technique, measure the reduction.
But human souls are not machines. As we explore in our article on Fixing Evidence-Based Practice, this reliance on short-term data ignores the long-term transformation of the personality.
The Scandal of Science:
We often trust “The Science” blindly, but studies like the STAR*D Scandal reveal that data is often manipulated to serve pharmaceutical interests. When we dig into the numbers, we find that the efficacy of antidepressants and short-term therapies is often vastly overstated.
Read More: When Evidence-Based Practice Goes Wrong: The STAR*D Scandal.
Part IV: The Brain Drain
The result of this systemic failure is a massive “Brain Drain” in the mental health field.
Talented, empathetic, and intuitive clinicians enter the field hoping to heal. They get jobs at agencies or hospitals, where they are forced to see 30+ patients a week, complete mountains of paperwork, and use rigid, manualized treatments that don’t work for complex trauma.
They burn out. And then, they leave.
They start private practices (like Taproot Therapy Collective) where they can opt out of the insurance game. In private practice, they are free to use deep, effective modalities like Brainspotting, Internal Family Systems (IFS), and Somatic Experiencing.
The Two-Tier System:
This creates a tragic inequality.
1. The Wealthy: Can afford to pay cash for experienced, private therapists who use deep, transformative methods.
2. The Public: Are left in the system, treated by overworked, under-trained staff who are restricted to “15-minute med checks” and manualized CBT.
Part V: The Irony of the Elite
Here is the ultimate irony: The very people who design these efficient, short-term systems do not use them for themselves.
Irvin Yalom, the famous existential psychiatrist, once asked a pointed question: “If CBT is so great, why do CBT therapists come to see me when they are in crisis?”
When a medical director, a hospital CEO, or a university dean goes through a divorce, a loss, or a dark night of the soul, they do not go to a clinic for 6 sessions of skills training. They go to a private practice. They seek out Jungian Analysis or Depth Psychology. They want someone who will listen to their soul, not just fix their “cognitive distortions.”
They know the truth: Efficiency is the enemy of intimacy. You cannot speed-run the healing of a human heart.
Conclusion: The Acorn Theory
In graduate school, I was shown a diagram of an acorn growing into an oak tree. It was meant to symbolize human potential. But the modern corporate system does not know how to grow oaks; it only knows how to manufacture lumber.
If we want to save this profession, we must stop pretending that “managed care” is care. It is management. We must return to the deep, messy, un-scalable work of sitting with another human being and witnessing their life. We must embrace the Modern Soul in all its complexity, rather than trying to reduce it to a billing code.
If this scares you, it should. But acknowledging the problem is the first step toward reclaiming the profession.
Further Reading on the Crisis in Therapy
Taproot Therapy Collective Podcast
The Failure of the Medical Model
Evidence-Based Practice is Broken: Let’s Fix It
The STAR*D Scandal: When Science Lies
The Illusion of Progress in Psychology
The Depth Alternatives
Jungian Therapy: Depth over Speed
Existential Therapy: Finding Meaning in Crisis
Healing the Modern Soul (Series)
Bibliography
- Newfield, C. (2016). The Great Mistake: How We Wrecked Public Universities and How We Can Fix Them. [cite_start]Johns Hopkins University Press. [cite: 2]
- Ginsberg, B. (2011). The Fall of the Faculty: The Rise of the All-Administrative University and Why It Matters. [cite_start]Oxford University Press. [cite: 3]
- Greenberg, G. (2013). The Book of Woe: The DSM and the Unmaking of Psychiatry. [cite_start]Blue Rider Press. [cite: 66]
- Harris, G. (2010). “Talk Therapy Dwindles as Psychiatrists Focus on Drugs.” [cite_start]New York Times. [cite: 1]
















0 Comments