
What if Bessel van der Kolk wrote a sequel to his influential book on trauma today?
Did you enjoy this article? Checkout the podcast here: https://gettherapybirmingham.podbean.com/
 e
e
If anyone is familiar with the book The Body Keeps the Score, by world renowned physician Bessel van der Kolk, the title of this article is obvious hyperbole. I have no idea if he would or what Bessel van der Kolk would write as a sequel to The Body Keeps the Score. I am sure his publishers have offered him an enormous cash advance for a follow up. For now that will have to stay between them.
The Body Keeps the Score was published almost a decade ago and its influence on the profession of trauma treatment has been profound. The book is different from other exposés on trauma treatment in that it is candid about the sordid history of trauma in psychology, and honest about the unfortunate current state of the profession of psychotherapy.
Another thing that makes the book a unicorn is that it is not only readable by lay people but also does not dumb anything down. It has been highly educational to seasoned therapists and patients alike. The confessional tone makes the author’s perspective as both a patient and provider of trauma treatment dually educational to both patients and providers. This is another reason for its profound success.

I’m not really sure how you suffix dutch names. Do you say “Mr. Kolk” or “Mr. van der Kolk”? Anyhow, if Bessel wrote a book today what would he say? How has his perspective on trauma treatment changed over the past ten years? What would he write about being the new future of trauma treatment after most of the predictions in his current book came true?
Based on his past professional decisions we could make certain guesses about what would happen if he had to write the book again today. He sits on several boards of both longer term treatment facilities and credentialing bodies of therapy modalities. That must tell us something about what he thinks about them.
Who knows where the future of brain based medicine for the treatment of trauma is going? If we are to figure it out together we need to listen to three things. The first is intuition both of the patient and the provider. I have always believed that providers need to be patients in the modalities that they train in, not simply receive the training. There is the “ah” of education that must be accompanied by the “ah hah” of direct experience. This is the part of therapy that too many providers are too quick to leave out.

I have been in more models of therapy than I can count, and when I did my first 40 minutes of brainspotting I knew that my life was forever different. Following my own intuition, I got phase 1 and phase 2 brainspotting training and began to ask patients if they wanted to try it. Almost all my patients had a positive result. Many had already made great progress with me in parts based models like IFS, somatic therapy, and with EMDR. I left it to the patient to choose, directly and indirectly, the treatment path that was right for them, and most people choose brainspotting. Demand for that brainspotting continued to grow in the area and requests for the treatment increased.
Listening to the intuition of the patient, the provider and the broader market is an important part of keeping the profession patient centered and not provider controlled. However intuition in a vacuum can be a problem. Dangerous fads have taken over the profession before because charismatic hustlers tricked the market into thinking they work. Research is an important part of the process too. We need to study new modalities.
Plenty of providers want to simply leave the future of the profession up to “research” without thinking about that statement further. Research does not create anything. Research isn’t visionary. Research measures the efficacy of things that other providers have already created. DBT, IFS, somatic experiencing EMDR, and brainspotting didn’t come waltzing out of a lab, they were created from a clinician’s intuition. If we wait for research to invent the next model of psychotherapy then that model will never come.
Good psychotherapy stays ahead of research by using research as an indicator of the future. Research helps us build neuroscientificaly plausible models based on what we do know. These create pathways to better models of the brain. This requires intelligence, intuition, and humility without objective certainty. Lack of certainty creates anxiety , but without facing it we will never build better models for healing.
If providers wait till research trickles through academic journals, to university curriculums, and then into major institutions they will likely be more than a decade behind the cutting edge of the profession. If I had waited for research to tell me to open a brainspotting based clinic I would still be waiting and Taproot would not exist yet. Research is an effective way to assess what exists but it can blind us if we are not willing to listen to ourselves or patients as providers. Predicting the future of psychotherapy practice means not only that we keep an eye on the current research, but also an ear to the ground about what has not yet been brought into the mainstream.
So back to the original question, but would Bessel van der Kolk include in a forward thinking book about psychotherapy today? I’m not sure but let’s look at the candidates and make a guess.
Brainspotting

Similar to EMDR, but more surgical in its focus, brainspotting is an eye movement therapy that uses an evolutionary glitch about how our brain processes visual information. Brainspotting works as well as other somatic trauma treatments like sensorimotor therapy and somatic experiencing, but it works incredibly fast. Brainspotting allows patients to feel and directly process the somatic and emotional damage caused by trauma and PTSD in a controlled way.
Brainspotting was a footnote in the EMDR community when The Body Keeps the Score came out. It is now one of the fastest modalities of trauma care out there. Many EMDR providers are pivoting to Brainspotting. Bessel van der Kolk has featured brainspotting guests on a couple of panels and boards he oversees. I feel confident that brainspotting would make the cut if there was a sequel today.
10/10.
Neurostimulation
Bessel van der Kolk mentions biofeedback in his book as a path forward for trauma treatment in his original book. Biofeedback, microcurrent neurofeedback (mcnf) and transcranial magnetic stimulation (tcms) were in their infancy a decade ago. Now there are more advanced applications of the technology. Like qEEG brain mapping and neurostimulation.
In qEEG brain mapping the frequencies of the brain neurons are mapped in order to understand diagnosis, symptoms and personality type of a patient. This can provide more information than psychometric testing or a diagnostic impression of a psychiatrist. The qEEG brain maps can give the patient objective proof of what is happening in the brain as a result of trauma and make PTSD easier for them to accept.
Neurostimulation uses the qEEg map to develop a neurostimulation plan. Patients wear a cap that mimics the neurons in the brain to “talk” to the brain and teach it how to heal. Unlike the methods mentioned in The Body Keeps the Score, neurostimulation is completely unique and can stimulate all parts of the brain in different ways. Neurons think in frequencies and neurostimulation uses these frequencies to help the neural cap merge with the brain and heal trauma.
I feel confident that Bessel would mention the updates to Neurostimulation and qEEG brain mapping in a sequel.
9/10
Psilocybin
Psychedelic mushrooms that dissolve ego consciousness have been used in healing rituals since the bronze age. When the brain becomes traumatized, thinking becomes rigid and reactionary. Psilocybin helps the brain reconnect with creativity and become more open to new ideas. It can heal trauma by opening new neural pathways in the brain and releasing maladaptive “stuck” connections.
Bessel van der Kolk did not say much about psychedelics in his first book even though they had been around for years. He hasn’t said much about them in the years since this book got published. He likely is more comfortable with more traditional medical practices. It is unlikely psilocybin would come up in the sequel. Leave the psychadelics to other authors like Michael Pollan.
3/10
Ketamine
Ketamine is an anesthesia drug that in mild doses relieves depression and anxiety and at larger doses is dissociating, hallucinogenic and similar to a psychedelic. Research is still out about the kinds of disorders it treats and the best way to administer it. Many of our patients have had good experiences receiving IV Ketamine at Southern Ketamine and Wellness treating treatment resistant conditions.
Although oral and nasal ketamine is hard to get in Alabama it is a growing option nationally. It will highly likely continue to grow in popularity as a treatment option. I think it is more than likely that it gets a passing mention in the sequel.
8/10
Micronutrients and Gut Health for Mental Health
 Research is continuing to show that our bodies are more than go carts that carry around our brains so that they can think. Our emotion and cognition is tied more intimately to our body and we must treat the whole body to change the way we think and feel. Micronutrient and gut health in psychology is one of the rare places where research is largely ahead of the clinical application of the profession.
Research is continuing to show that our bodies are more than go carts that carry around our brains so that they can think. Our emotion and cognition is tied more intimately to our body and we must treat the whole body to change the way we think and feel. Micronutrient and gut health in psychology is one of the rare places where research is largely ahead of the clinical application of the profession.
Research continues to show that the way we metabolize energy and nutrients in our gut affects the neurotransmitters in our brain. It makes sense if we do not have the precursors, or building blocks, to make neurotransmitters in our diet. How do we expect them to get made? Research shows that gut bacteria, like lactobacillus and bifidobacterium, can reduce the need for medication or make it more effective for treatment related conditions.
Micronutrient based mental health care is more than just “taking vitamins”. Instead it is about identifying nutrients that have a synergistic effect or react more effectively and sometimes completely differently when taken together in the right amount. For example Quercetin, N-A-C (n-acetyl cysteine) and Vitamin C boost the universal antioxidants o-quinone and glutathione. This combination can reduce the risk of many physical and mental health issues even protecting against Covid 19. Taking any of the parts alone does not have this effect. We think about nutrition as more of a list of “daily values” and milligrams when we really should think of it as more of a recipe.
Bessel van der Kolk mentions nutrition a bit but doesn’t seem to have explored these avenues much since the book came out. It is a toss up whether or not this would be mentioned in the sequel.
6/10
Stellate Ganglion Block
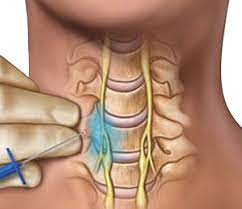 The stellate ganglion block is a minimally invasive surgical procedure that has been around for over 100 years. In the past twenty years it has started to be used more and more for trauma. In the SGB procedure a MD injects anesthesia into the nerves between the C6 and C7 vertebrae. This part of the “body brain” regulates our stress and emotional responses. It is what gets overloaded during trauma and leaves the body and the emotional system still experiencing a traumatic event from years ago.
The stellate ganglion block is a minimally invasive surgical procedure that has been around for over 100 years. In the past twenty years it has started to be used more and more for trauma. In the SGB procedure a MD injects anesthesia into the nerves between the C6 and C7 vertebrae. This part of the “body brain” regulates our stress and emotional responses. It is what gets overloaded during trauma and leaves the body and the emotional system still experiencing a traumatic event from years ago.
The injection of the anesthesia helps the stellate ganglion “forget and reset” how it reacts to emotion physically and cognitively. I have talked to several providers who use SGB for PTSD. When the procedure works the effect on the client is similar to brainspotting but takes place immediately. Because it is technically a surgery the expense of this procedure can be prohibitive.
Would Bessel van der Kolk mention this? Perhaps. Recent research would make it a hard thing to omit from the future of trauma treatment.
7/10
Mental Health Treatment Fusing with Physical Therapies
 So many of the treatments that work for trauma have a focus on the body and bringing the patient’s “body brain” back into equilibrium. Somatic Experiencing, IFS and Sensorimotor psychotherapy seem to be growing in popularity, slowed by the long training and certification process. Bessel van der Kolk has spoken positively of all of these models and participates in joint ventures with the founders. The Body Keeps the Score mentions using creativity, using the body, and breaking the self into a series of parts to get a n outsider perspective as the throughline in all the most effective models for trauma.
So many of the treatments that work for trauma have a focus on the body and bringing the patient’s “body brain” back into equilibrium. Somatic Experiencing, IFS and Sensorimotor psychotherapy seem to be growing in popularity, slowed by the long training and certification process. Bessel van der Kolk has spoken positively of all of these models and participates in joint ventures with the founders. The Body Keeps the Score mentions using creativity, using the body, and breaking the self into a series of parts to get a n outsider perspective as the throughline in all the most effective models for trauma.
With these models now in the mainstream, what does the future fusion of mental and physical health care look like? How will the body continue to enter the psychotherapy room? Trauma can make it difficult for therapy patients to feel their bodies and connect with them. This can make using the body in therapy difficult. Often patients need help regulating the body physically before they can regulate it emotionally and this means they need a physical type of therapy.
We have found at Taproot Therapy that patients that get stuck in brainspotting and somatic modalities have great results when seeing myofascial release, dry needling and ROLF massage practitioners. These models of physical therapy analyze posture. In doing so they can help patients understand what effect trauma and development have on the way they hold themselves. By changing and becoming aware of posture and muscular reaction to emotion we can overcome the somatic and unconscious realities affecting our lives.
Myofascial and ROLF massage both try to reset muscle systems, not massage sore areas. They are trying to “reset” the way that we hold emotion physically from the body in the same way that brainspotting and neurofeedback “reset” the way the body holds emotion from the brain. Many times the muscle tension is so deep in a patient’s muscle system that the provider cannot “see” it and help the patient understand it without physical touch.
Using the body in psychotherapy is not entirely new. Wilhelm Reich split from the original psychoanalytic school when Freud would not consider his idea about “body armoring”. Reich would poke spots of muscle tension to elicit emotional reactions. Practitioners like Arnie Mindell use physical techniques and touch to help patients release emotion from the body in his process psychotherapy modality.
I personally think that holding the physical and emotional with separate providers is the best approach. A single provider being a safe space for emotional reprocessing but also using physical touch seems like too murky of a boundary for me. We refer our patients to other myofascial release and ROLF providers for physical work. We would love to have one at Taproot one day also!
So would Bessel van der Kolk include the continued fusion of mental and physical health care in a sequel? I mean, he wrote a book called The Body Keeps the Score. I’m sure he would.
10/10
Bibliography:
van der Kolk, B. A. (2014). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Penguin Books.
Ashton, M. (2023). What if Bessel van der Kolk Wrote a Sequel to his Influential Book on Trauma Today? GetTherapyBirmingham.com.
Bisson, J. I., Roberts, N. P., Andrew, M., Cooper, R., & Lewis, C. (2013). Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database of Systematic Reviews, (12). https://doi.org/10.1002/14651858.CD003388.pub4
Emerson, D., Sharma, R., Chaudhry, S., & Turner, J. (2009). Yoga Therapy in Practice: Trauma-Sensitive Yoga: Principles, Practice, and Research. International Journal of Yoga Therapy, 19(1), 123-128. https://doi.org/10.17761/ijyt.19.1.h6476p8084vowu46
Hossain, M. M., Purohit, N., Sharma, R., Bashir, K., & Sultana, A. (2021). Impacts of the COVID-19 Pandemic on the Mental Health of Healthcare Workers: A Narrative Review. Asian Journal of Psychiatry, 54, 102271. https://doi.org/10.1016/j.ajp.2020.102271
Iribarren, J., Prolo, P., Neagos, N., & Chiappelli, F. (2005). Post-Traumatic Stress Disorder: Evidence-Based Research for the Third Millennium. Evidence-Based Complementary and Alternative Medicine, 2(4), 503-512. https://doi.org/10.1093/ecam/neh127
Lipov, E. G., & Lipov, S. (2018). Stellate Ganglion Block for the Treatment of Post-Traumatic Stress Disorder: A Case Report and Review of the Literature. Anesthesiology and Pain Medicine, 8(5). https://doi.org/10.5812/aapm.81821
Mulvaney, S. W., McLean, B., & de Leeuw, J. (2014). The Use of Stellate Ganglion Block in the Treatment of Post-Traumatic Stress Disorder: A Review of the Literature. Pain Medicine, 15(6), 1122-1130. https://doi.org/10.1111/pme.12422
Further Reading:
Briere, J., & Scott, C. (2015). Principles of Trauma Therapy: A Guide to Symptoms, Evaluation, and Treatment. SAGE Publications.
Fosha, D., Siegel, D. J., & Solomon, M. F. (Eds.). (2009). The Healing Power of Emotion: Affective Neuroscience, Development & Clinical Practice. W. W. Norton & Company.
Geller, S. M., & Porges, S. W. (2014). Therapeutic Presence: Neurophysiological Mechanisms Mediating Feeling Safe in Therapeutic Relationships. Journal of Psychotherapy Integration, 24(3), 178-192. https://doi.org/10.1037/a0037511
Hesse, E. (2008). The Adult Attachment Interview: Protocol, Method of Analysis, and Empirical Studies. In J. Cassidy & P. R. Shaver (Eds.), Handbook of Attachment: Theory, Research, and Clinical Applications (2nd ed., pp. 552-598). Guilford Press.
Levine, P. A. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. North Atlantic Books.
Siegel, D. J. (2012). The Developing Mind: How Relationships and the Brain Interact to Shape Who We Are (2nd ed.). Guilford Press.
Schore, A. N. (2012). The Science of the Art of Psychotherapy. W. W. Norton & Company.






















0 Comments