
The Complex Reality of EMDR in Clinical Practice
Eye Movement Desensitization and Reprocessing (EMDR) occupies a unique and controversial position in the landscape of trauma therapy. While some practitioners report remarkable results, researchers often express skepticism about its mechanisms calling it a purple hat therapy and effectiveness. This divide between clinical experience and research findings reveals important truths about how we understand and treat trauma.
Understanding EMDR’s Mixed Reception
EMDR therapy demonstrates effectiveness for approximately 30% of trauma survivors—a significant portion, though not the universal solution some proponents claim. This selective effectiveness creates challenges for research validation, as studies consistently find EMDR to be “slightly less effective or more effective than nothing,” leading to mixed conclusions about its clinical value.
The therapy’s reputation suffers from what many describe as a “culty” atmosphere among some practitioners. This fervent advocacy, while born from genuine clinical successes, often alienates researchers and creates barriers to serious scientific investigation. The gap between clinician enthusiasm and researcher skepticism reflects deeper issues in how we study and understand psychotherapy effectiveness.
The Limitations of Traditional Trauma Classification
A critical factor in understanding EMDR’s variable effectiveness lies in the inadequacy of current diagnostic frameworks. The DSM-5’s approach to post-traumatic stress disorder fails to capture the nuanced differences between trauma types that experienced clinicians observe daily.
Consider the distinct presentations of trauma:
Dissociative-type trauma manifests differently from flashbulb-experiencing trauma. A person who dissociates during traumatic memories requires different therapeutic approaches than someone experiencing vivid, intrusive flashbacks.
Relational trauma embedded in early attachment disruptions presents unique challenges compared to single-incident traumas. The body stores these experiences differently, and therapeutic interventions must adapt accordingly.
Somatic presentations where emotions remain “stuck” in the body, unrecognized and unprocessed, respond to different modalities than cognitive or visual traumatic memories.
These distinctions, readily apparent to skilled clinicians, remain poorly captured by standardized diagnostic criteria. This classification problem directly impacts research outcomes—studies that fail to differentiate between trauma types inevitably produce mixed results.
The Neuroscience Gap: Why 1980s Theories No Longer Suffice
Francine Shapiro’s original theories about bilateral stimulation and REM sleep processes represented reasonable hypotheses for their time. However, five decades of neuroscience research have revealed a more complex picture of how eye movements interact with memory processing and emotional regulation.
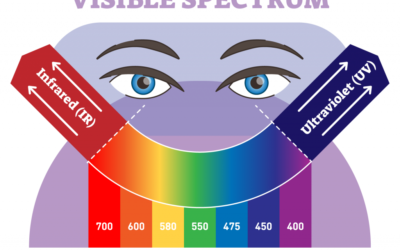
Modern understanding of the visual system reveals that 90% of the optic nerve bypasses conscious visual processing, wrapping around the brainstem to create immediate subcortical responses. This means we react to visual stimuli before we consciously “see” them—a finding with profound implications for eye-position therapies.
Research in fields outside traditional psychology—including advertising, user interface design, and primate behavior studies—provides compelling evidence for the relationship between eye position, pupil dilation, and emotional states. During memory reconsolidation, specific eye positions correspond to different types of memory retrieval, observable through theta wave patterns in QEEG studies.
EMDR as a Bridge to More Effective Therapies
Perhaps EMDR’s greatest contribution lies not in its direct effectiveness but in opening the door to more refined approaches. Brainspotting, developed by David Grand, builds on EMDR’s insights while achieving higher success rates—approximately 80% of clients experience immediate, noticeable effects.
These newer approaches recognize that eye position matters under specific conditions. Clinicians trained in brain spotting observe phenomena that skeptics dismiss: dramatic pupil dilations that mirror those seen in neurological conditions, immediate exhaustion and fugue-like states, and the “strobe light” effect of rapidly dilating pupils during trauma processing.
Emotional Transformation Therapy, developed by Dr. Steven Vazquez, pushes these observations even further. His documented case of a patient with occipital blindness who still responded to visual stimuli through intact subcortical pathways challenges our understanding of how visual processing affects emotional regulation.
The Research-Practice Divide in Trauma Therapy
The structure and funding of psychological research in the United States creates systematic barriers to understanding these therapies. Research priorities often misalign with clinical realities, and researchers without extensive clinical experience may miss subtle but crucial therapeutic phenomena.
Meanwhile, market forces provide a different form of validation. When therapists—typically not wealthy individuals—invest thousands of dollars in training for therapies that lack institutional support, they signal confidence born from observed effectiveness. The proliferation of eye-movement-based therapies in private practice, despite limited research validation, suggests clinical value that traditional research methods fail to capture.
Moving Forward: Integration Rather Than Dismissal
The question “Is EMDR pseudoscience?” misses the more important consideration: How can we understand and refine what works about EMDR while developing more effective interventions?
EMDR’s selective effectiveness points toward the need for:
- More sophisticated trauma classification systems that recognize neurobiological differences between trauma types
- Research methodologies that can capture subtle clinical phenomena
- Integration of findings from neuroscience, vision research, and clinical practice
- Recognition that outdated theoretical frameworks don’t invalidate observed clinical effects
The therapy’s role in pioneering eye-movement-based interventions remains significant, even as newer approaches surpass its effectiveness. Understanding EMDR’s limitations and contributions helps advance the field toward more precise, effective trauma treatments.
References
Shapiro, F. (2001). Eye Movement Desensitization and Reprocessing (EMDR): Basic Principles, Protocols, and Procedures (2nd ed.). Guilford Press.
van der Kolk, B. A., Spinazzola, J., Blaustein, M. E., Hopper, J. W., Hopper, E. K., Korn, D. L., & Simpson, W. B. (2007). A randomized clinical trial of eye movement desensitization and reprocessing (EMDR), fluoxetine, and pill placebo in the treatment of posttraumatic stress disorder: Treatment effects and long-term maintenance. Journal of Clinical Psychiatry, 68(1), 37-46.
Grand, D. (2013). Brainspotting: The Revolutionary New Therapy for Rapid and Effective Change. Sounds True.
Davidson, P. R., & Parker, K. C. (2001). Eye movement desensitization and reprocessing (EMDR): A meta-analysis. Journal of Consulting and Clinical Psychology, 69(2), 305-316.
Corrigan, F. M., Grand, D., & Raju, R. (2015). Brainspotting: Sustained attention, spinothalamic tracts, thalamocortical processing, and the healing of adaptive orientation truncated by traumatic experience. Medical Hypotheses, 84(4), 384-394.
Lee, C. W., & Cuijpers, P. (2013). A meta-analysis of the contribution of eye movements in processing emotional memories. Journal of Behavior Therapy and Experimental Psychiatry, 44(2), 231-239.
Vazquez, S. (2014). Emotional Transformation Therapy: An Interactive Ecological Psychotherapy. Rowman & Littlefield.
Jeffries, F. W., & Davis, P. (2013). What is the role of eye movements in eye movement desensitization and reprocessing (EMDR) for post-traumatic stress disorder (PTSD)? A review. Behavioural and Cognitive Psychotherapy, 41(3), 290-300.
Solomon, R. M., & Shapiro, F. (2008). EMDR and the adaptive information processing model: Potential mechanisms of change. Journal of EMDR Practice and Research, 2(4), 315-325.
Schubert, S. J., Lee, C. W., & Drummond, P. D. (2011). The efficacy and psychophysiological correlates of dual-attention tasks in eye movement desensitization and reprocessing (EMDR). Journal of Anxiety Disorders, 25(1), 1-11.
Armstrong, M. S., & Vaughan, K. (1996). An orienting response model of eye movement desensitization. Journal of Behavior Therapy and Experimental Psychiatry, 27(1), 21-32.
van den Hout, M. A., & Engelhard, I. M. (2012). How does EMDR work? Journal of Experimental Psychopathology, 3(5), 724-738.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton & Company.
LeDoux, J. (2015). Anxious: Using the Brain to Understand and Treat Fear and Anxiety. Viking.
Lanius, R. A., Vermetten, E., & Pain, C. (Eds.). (2010). The Impact of Early Life Trauma on Health and Disease: The Hidden Epidemic. Cambridge University Press.
















0 Comments