
Executive Summary: The Agency Trap
The Clinical Dilemma: Child therapy often fails not because of the therapist’s lack of skill, but because of the child’s lack of legal and physical agency. Treating a child in an abusive home is often treating the symptom while the system remains toxic.
Key Concepts:
- The Identified Patient: In family systems theory, the child is often the “symptom bearer” for the family’s dysfunction.
- Reparenting: Adult therapy allows for a “Corrective Emotional Experience” where the therapist models the consistent, protective parent the client never had.
- Agency vs. Plasticity: Child therapists trade agency for plasticity (the child can change, but can’t leave). Adult therapists trade plasticity for agency (the adult can leave, but change is harder).
The Pivot: Moving to adult therapy allows the clinician to work with patients who have the power to change their environment, turning therapy from “coping with abuse” to “healing from abuse.”
Why I Don’t Work With Kids Anymore: The Ethics of Agency and the Pain of Witnessing

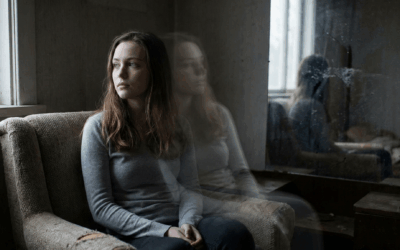
Early in my career, I aspired to be a “universal donor”—a therapist who could sit with anyone, regardless of age, background, or pathology. I believed that empathy was a skeleton key that could unlock any door. However, the brutal reality of clinical practice often dismantles our early idealism. A turning point came for me on a freezing Saturday night, when I found myself on the phone with a 14-year-old patient.
He was standing outside in the bitter cold because his mother had locked him out of the house during a manic episode. He called me, his voice trembling not just with cold but with the desperate, primal fear of abandonment, hoping I could pick him up and save him. In that moment, the structural impotence of child therapy crashed down on me. Unlike my adult patients, I couldn’t tell him to set a boundary. I couldn’t advise him to leave. I couldn’t help him deconstruct his resistance to change because he wasn’t the problem.
My role as a mandated reporter meant I could—and did—call Child Protective Services (CPS). But any therapist who has worked in the system knows that a call to CPS is rarely a magic wand. It often results in a cursory investigation, a warning to the parents, and a child who is now in even more danger because the abuser knows they “snitched.” That Saturday, as I waited on the phone for the police to arrive, listening to the wind howl through the receiver, I made the difficult decision to stop working with children. I realized that my capacity to sit with helplessness had a limit, and that limit was the legal inability to save a child from their own parents.
The Identified Patient and the Closed Loop
In Family Systems Theory, there is a concept known as the “Identified Patient.” This is the family member—usually a child or adolescent—who manifests the symptoms of the family’s collective dysfunction. The parents bring the child to therapy saying, “Fix him,” while remaining completely unwilling to examine the toxic marriage, the addiction, or the neglect that is causing the child’s behavior.
Treating children often felt like being a mechanic trying to fix a car while the owner is actively smashing the engine with a sledgehammer. You can tune the carburetor (teach coping skills), but as long as the hammer creates chaos (the home environment), the car will never run.
This is why I pivoted to adults. With an adult, the locus of control shifts. Even if an adult is trapped in a domestic violence situation or a crushing addiction, they possess the legal and developmental capacity to leave. We can work on the “Why” of their staying. We can analyze the “Parts” that are terrified of independence. The barrier is psychological, not structural. With a child, the barrier is often literal: they cannot sign a lease; they cannot drive away; they belong to the system that hurts them.
Reparenting: The “Corrective Emotional Experience”
In my work with adult survivors of childhood trauma, I often employ psychodynamic techniques that involve a process known as Reparenting. This is not about literally becoming their parent, but about providing a relational template that contrasts with the abusive one they grew up with. As Heinz Kohut famously explored in The Analysis of the Self, the therapist must function as a “Selfobject”—a mirror that reflects the patient’s worth until they can hold it themselves.
A key aspect of this work is teaching patients that their needs are not dangerous. Many adults who experienced neglect learned early on that having a need resulted in rejection or violence. Therefore, they developed a “hyper-independent” or avoidant attachment style. They believe that asking for help is a moral failing.
By being available to patients during crises—within boundaries, but with consistency—therapists can challenge these entrenched beliefs. When a patient calls in distress and expects to be yelled at (transference from the parent), but instead receives calm, regulated support, a neural pathway changes. They learn that the “Bad Object” (the abusive parent) is not the only model of authority in the world. This is what Franz Alexander called the “Corrective Emotional Experience.”
The Paradox of Plasticity vs. Agency
I once shared my frustration with a colleague who specializes in child therapy. I told him, “I can’t do it. I can’t watch them get hurt and be unable to stop it.”
He looked at me with a wry, sad smile and said, “That’s funny. I don’t know how you work with adults. With kids, the concrete is still wet. We can shape it. With adults, I feel like I’m trying to chip away at hardened cement. I feel like it’s already too late.”
His words struck a chord. We were grappling with the same existential limitation of our profession, but from opposite ends of the timeline.
* The Child Therapist: Has High Plasticity (the brain is changing rapidly) but Low Agency (the patient cannot control their environment).
* The Adult Therapist: Has High Agency (the patient can leave) but Low Plasticity (the patterns are deeply entrenched).
For me, providing therapy to adults became a way to help them heal from a past I couldn’t alter. I realized I am better at jackhammering the cement than I am at watching the wet concrete get stomped on. By working with the adult, I am essentially working with the child they used to be—the “Inner Child” or “Exile” in Internal Family Systems (IFS) terms. I can finally give that child a voice, a defense, and an escape route, even if it is thirty years late.
The Power of “Being With”
Ultimately, whether we work with the 14-year-old in the cold or the 40-year-old remembering the cold, the core of the work is Witnessing.
Trauma is not just the bad event; it is the experience of being alone with the bad event. As D.W. Winnicott noted, the child needs a “holding environment” to integrate their experiences. When that holding environment fails, the psyche fragments.
Therapy provides a delayed holding environment. By creating a safe, non-judgmental space (what Carl Rogers called “Unconditional Positive Regard”), we allow the patient to bring the fragmented parts of themselves out of the shadows. We cannot change the history. We cannot erase the abuse. But we can change the story of the abuse. We can move the patient from “I was hurt because I was bad” to “I was hurt because I was vulnerable, and I survived.”
I stopped working with children not because I don’t care about them, but because I care too much to watch them suffer without the power to intervene. I choose to work with the survivors—the ones who made it out—to help them realize that the war is over, and they don’t have to be soldiers anymore.
Bibliography
- Kohut, H. (1971). The Analysis of the Self. International Universities Press.
- Winnicott, D. W. (1965). The Maturational Processes and the Facilitating Environment. International Universities Press.
- Rogers, C. R. (1951). Client-Centered Therapy. Houghton Mifflin.
- Herman, J. L. (1992). Trauma and Recovery. Basic Books.
- Miller, A. (1981). The Drama of the Gifted Child. Basic Books.














0 Comments