
Key Points and Main Ideas:
- Shift in psychiatric practice from hour-long psychotherapy sessions to brief medication-focused appointments.
- Criticism of the current trend of diagnosing and prescribing medication without thorough assessment of patients’ life circumstances.
- Economic pressures forcing psychiatrists and psychologists into more lucrative areas of practice, away from traditional psychotherapy.
- Increased control of mental healthcare by insurance companies and medical directors who often lack experience in psychotherapy.
- Criticism of graduate education in psychotherapy, focusing on its high cost and perceived lack of practical training.
- The corporatization of universities and its negative impact on the quality of education, particularly in mental health fields.
- Overemphasis on manualized therapy models (like CBT and DBT) in graduate education at the expense of other therapeutic approaches.
- The gap between what is taught in graduate programs and the skills needed for effective private practice.
- Concern that current mental health practices focus more on managing symptoms than on fostering personal growth and insight.
- The trend of experienced psychotherapists moving to private practice, leaving institutions with less experienced practitioners.
- Critique of the short-term, profit-driven approach to mental healthcare in corporate and academic settings.
- The irony that many healthcare managers and educators seek private psychotherapy despite not valuing it in their professional roles.
- Concern about psychotherapy becoming a luxury available only to the upper and middle classes.
- Call for acknowledgment and discussion of these issues within the mental health community.
- The need for a more comprehensive, growth-oriented approach to psychotherapy that goes beyond symptom management.
Why is Psychotherapy Getting Worse:
Psychiatrists used to spend an entire hour with their patients doing psychotherapy. For the majority of the profession, up until the most recent decades this is what they did. The proposition seems outrageous now. Psychiatrists that are still practicing psychotherapy for a whole hour now are usually pushing eighty. The most common complaints that I hear from patients are that they give up on medication after their former psychiatrist wrote a script in the first and last five minutes of their first session.
I hate to side with patients against my peers in the mental health profession, but many times patients are absolutely right. Five minutes is not enough to figure out if anxiety, depression and other symptoms are a normal and even healthy response to events or environment. Many patients I see who complain that their anxiety medications are “not working”, I discover in the first session are victims of ongoing household abuse, suffering with complex grief, or other factors that cannot be drugged away. It is not enough as a clinician to check a box of existing symptoms but often more important to “get under” the symptoms and discover their origin and function in a patient’s psyche. I keep a long list of all of the psychiatrists nearby that do comprehensive diagnosis, however I have to warn patients that they will likely have to wait several months to see these doctors. The realities of corporate encroachment on medicine and education, namely through reliance on private insurance and the cost of education, have forced many psychiatrists and even many clinical psychologists into more lucrative areas of private practicing like psychometrics, management roles, and prescribing. Even well meaning professionals are drowning in student loans and forced to reckon with the modern economic realities of the profession. Doctors have to work for years in for-profit institutions before they even have the options of going into private practice. 89% of psychiatrists solely used drug therapy in 2010 compared with 81% in 2002 and 54% in 1988. However, it should be pointed out that the American Medical Association has been heavily involved in the economic trends that have decreased the quality and access of mental health care to patients and restrict options to psychotherapy practitioners.
Most of the board members and medical directors for these private insurance companies that exercise such vast control over the mental healthcare industry are in fact MD’s. The same MD’s that decline to practice, even learn to practice, or even go to psychotherapy. I do not know the numbers for how many MD’s even encounter psychotherapy in their psychiatric rotations, but I promise you they are dismal. If the AMA wants to exercise this much control over the practice of psychotherapy, perhaps its members should learn to practice it first. Why do people who never bothered to learn or practice psychotherapy write the rules for a medicine they are largely ignorant of? So if the doctors are pulling out of psychotherapy, surely the Universities that teach the professionals that actually practice therapy are picking up the slack, right? When I meet with recent graduates looking for work out of school I always ask them the same question “What is the last thing you learned that helped you practice therapy?” Most ALC’s and LMSW’s will answer with a blank stare followed by some statistic or factoid from a grad school test question. Rarely, interesting candidates will tell me passionately about about existentialism, depth psychology, somatic work, eye movement therapies or some other discovery they have made and applied to work with patients. Almost never will this information have come from their graduate work. So what is it that universities and actually doing?
Making money would be the short answer. The cost of a public university education is now 3,009% more expensive than it was in 1970 after adjusting for inflation. That four year degree that your parents talk about flipping burgers to pay for cost, on average, $405. The average total cost of a 4 year degree is now $122,000 (https://educationdata.org/average-cost-of-college/). So where does the money go? It doesn’t go to professors, which we will get into later. It certainly isn’t making better psychotherapists. So where does it go? This is a big question, and not the focus of this article, so I will be brief. As public colleges became run more like for profit corporations this money went to dubious education technology platforms that are extremely unpopular with students. It also goes to a surplus of deans and university executives that now function more like CEO’s. Gone are the days when each school had a dean. Browse the website of any public university and you will see and endless scroll of titles like: Dean of Environmental Student Leadership Engagement for Strategic Minority Fundraising. Most schools won’t even list the university executives on the same page of the website to obfuscate how many leadership roles that they actually pay for. You have to click through to each individual college or schools website to find them all like a digital scavenger hunt. So how does this affect psychotherapy?
For one it is becoming more and more difficult for practitioners to afford the degrees that actually let them get licensed to practice the profession. The amount of expense and capacity for debt that it takes to go college keeps talented professionals out of the profession and makes the field less of a meritocracy. This is of course not just hurting the profession of psychotherapy, but also many other professions that rely on a master’s degree or more education for the terminal degree of licensure. More importantly, the quality of the education has suffered as the language of corporate America has crept into the administrative halls of American Universities. Increasingly board meetings refer to “deliverables” “profit loss ratios” and, most ghastly, many deans even refer to retained and graduated students as “products.” Of course, academic standards must be sacrificed to meet this new metric, and the mission of the organization changes. Assessing students on whether they know the information required to do the job or have the tools to innovate and self educate after college might delay the launch of the “product.” Surprisingly, university’s reluctance to hire professors that have a Phd hasn’t diminished their desire to sell you a Phd. Campuses are expanding and promoting more doctorate programs to therapists than ever before. I once had an economics professor defend this new model of education to me as “more efficient” and the cost of education as a result of “supply and demand”. “And what happens to demand when universities no longer hire Phd grads they are selling?” I asked him. He didn’t have an answer. The corporate education system had found a way to make you a more valuable product. It didn’t matter who that product was for exactly.
When I was in graduate school it was no secret that many of the students in my program would not, could not (and didn’t) ever work in the field. This reality was not ever seen as an impediment to graduating these students “to completion”, even if it took them a few extra years. It was clear that adjunct professors that were often seeing the material for the first time while they taught it to me. Tenure track professors are a threat to the profitability of the new academic model, so they now make up about only 1/4 of the faculty at American colleges. Adjuncts that can’t do psychotherapy often can’t teach it and those that can do therapy are often limited by curriculum that they have no control over. I would like to think that my experience was an exception to the norm, but anyone who has ever tried to hire or train earnest and well-meaning applicants straight out of graduate school can attest to how little they know about psychotherapy.
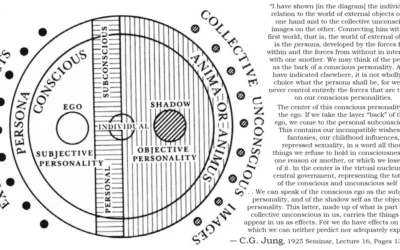
Even in colleges that do care about the success of their students after graduation, “success” often means immediate employability. This means that education largely prepares students to work in other institutions and trains students in the manualized models of therapy institutions prefer. It is terrifying to me that many recent graduates think that CBT therapy is therapy. When you ask recent graduates about their personal style, model, or theoretical orientation you will often get another blank stare followed by a description of a CBT or DBT intervention. This is so scary to me as a therapist, because after 8 years of obsessively absorbing audio books lectures and readings I realize that I still know almost nothing about the breadth, scope, and history of this profession. Recently I discovered a series of talks done by Jungians in the seventies during a week long conference. Why didn’t anyone tell me this stuff in graduate school?! was my first thought. I eagerly shared the techniques with my colleagues who were blown away. “This is like somatic experiencing forty years before it was invented,” one colleague told me.
IFS, schema therapy, voice dialogue, somatic experiencing, brainspotting, EMDR, emotion focused, humanistic, analytical psychology… the list goes on and on. Some of these models are mentioned in passing during a survey course and then never touched on again while adjuncts teach students how to find cognitive distortions and lead DBT groups. And yet, these are the models that are practiced, and often integratively, by the majority of private practice practitioners. But alas, these models often deal with the intangible, highly personal and not formulaic parts of therapy that are no longer valued by the medical or academic community. The corporatization of these entities has forced out anything that is not tangible, measurable and objective. With it, it has forced the best and most capable practitioners out of the institutions and into private practice.
If I had a nickle for every time I heard “You learn about that part of therapy in the field” when I was in graduate school, I could have made a dent in the cost of my tuition. If graduate schools are no longer teaching students the parts of therapy that they need for private practice, then why are we requiring students to go to them? Students could just learn during their apprenticeships “in the field.” The profit-seeking model of education is no longer weeding out the students that can’t do therapy, nor teaching the ones that can how to do it beyond the barest and most formulaic framework.
In graduate school we were shown a diagram of an acorn connected with an arrow to a small tree and then an oak tree to represent human aging across the life span. It was implied that humans went through different phases in life finally aging gracefully into an oak tree. The parts of psychotherapy that are needed to facilitate this process of growth, introspection, and identity development were not taught to us though. It was simply understood that peoples insight, maturity and wisdom develop naturally, and it was our job merely to reduce specific “symptoms” at different parts of this process.
Sadly our world is evidence that this idea is not true. I see fifty year old women pretending to be twenty one. I see eighty year old men who have never accepted the fact that we die. I see a majority of patients too scared, worn down, or lost to listen to the “acorn” latent within themselves and foster its growth. Without better psychotherapy, most of us will die a sapling. I am reminded of an interview that Irvin Yalom, arguably the founder of existential psychotherapy, did in 1996 where he asked, “If cognitive behavioral therapy works for everything then why do CBT therapists come to see me and not another CBT therapist?”.
The goal of corporate healthcare has become managing not curing trauma. What cannot be briefly cured is medicated. Academic institutions and medical institutions have built systems designed to insulate themselves from change. Supervisors are often rewarded with promotion for not pointing out, or worse not being able to see, systemic problems. The goal of corporate healthcare has become short term and shortsighted care as a preparation for a medication regimen. Insight, growth, and human connection are not objective and not profitable enough. Short-term thinking, ignoring cognitive dissonance, organizational ideological hypocrisy is encouraged where they increase profitability.
Hey, wait a minute! Aren’t those the same things we encourage our patients not to do from our offices in private practice? No wonder the managers of these institutions don’t see the value of “our kind” of psychotherapy. Except… they do. Open up a private practice and one by one they will walk through your door. So where does that leave us?
The doctors choosing the direction of the profession and are not practicing psychotherapy. The teachers teaching psychotherapy aren’t teaching it. The students learning psychotherapy aren’t learning it. The professionals practicing psychotherapy aren’t working in the hospitals and the colleges anymore. Where does that leave psychotherapy? As a luxury curiosity of the upper and increasingly shrinking middle class? All parts of this system seem to know these things but everyone is afraid to say it. Maybe that’s where we start. *Ahem “This scares me does it scare you?” What should we do about it?
Read More About Evidence Based Practice and Research Psychology:
Lessons from the STAR*D Scandal
The Corporatization of Healthcare
Incentives in Evidence Based Practice
Healing The Modern Soul Series Part 1 Part 2 Part 3 Part 4 Healing the Modern Soul Appendix
Bibliography:
Yalom, Irvin D. The Gift of Therapy: An Open Letter to a New Generation of Therapists and Their Patients. Harper Perennial, 2017.
Maté, Gabor. When the Body Says No: Exploring the Stress-Disease Connection. Wiley, 2011.
Shedler, Jonathan. “The Efficacy of Psychodynamic Psychotherapy.” American Psychologist, vol. 65, no. 2, 2010, pp. 98-109.
Greenberg, Gary. The Book of Woe: The DSM and the Unmaking of Psychiatry. Blue Rider Press, 2013.
Breggin, Peter. Toxic Psychiatry: Why Therapy, Empathy and Love Must Replace the Drugs, Electroshock, and Biochemical Theories of the “New Psychiatry”. St. Martin’s Press, 1991.
Further Reading:
Darden, Victoria A. “The Corporate Transformation of Higher Education.” Journal of Interdisciplinary Studies, vol. 22, no. 1/2, 2009, p. 51-68.
Newfield, Christopher. The Great Mistake: How We Wrecked Public Universities and How We Can Fix Them. Johns Hopkins University Press, 2016.
Ginsberg, Benjamin. The Fall of the Faculty: The Rise of the All-Administrative University and Why It Matters. Oxford University Press, 2011.
Slaughter, Sheila, and Gary Rhoades. Academic Capitalism and the New Economy: Markets, State, and Higher Education. Johns Hopkins University Press, 2004.
Fazackerley, Anna. “University Executive Pay: The Inside Story.” The Guardian, 23 Nov. 2018.
Norcross, John C., and Bruce E. Wampold. “Evidence-Based Therapy Relationships: Research Conclusions and Clinical Practices.” Psychotherapy, vol. 48, no. 1, 2011, pp. 98–102.
Barkham, Michael, and Gillian E. Hardy. “The Evaluation of Psychological Therapies: Developing a Rigorous Approach.” Clinical Psychology & Psychotherapy, vol. 1, no. 1, 1994, pp. 3–14.
Levant, Ronald F. “Psychotherapy Research and the Revitalization of Psychology.” Professional Psychology: Research and Practice, vol. 36, no. 4, 2005, pp. 372–383.









0 Comments