")
What is it that Brainspotting is doing in the brain?
We know well the psychosis needs to be medicated, and that medication is the fastest way to treat schizophrenia. Our lack of understanding how it works cannot get in the way of us providing effective evidence based solutions that do work.
Here are some of the prevailing theories about why brainspotting works:
Traumatic Associations in the Subcortical Brain:
Traumatic incidents can indeed lead to the formation of strong associations in the subcortical brain structures, particularly the amygdala. The amygdala is central to emotional processing and is responsible for recognizing and responding to emotional stimuli, especially those perceived as threats. When a traumatic event occurs, the amygdala may associate various stimuli (e.g., sights, sounds, smells) with extreme somatic and emotional reactions. These associations are part of the brain’s survival mechanism, designed to help us respond quickly to threats.
Difficulty Regulating Mood and Emotional States:
Trauma can disrupt the brain’s ability to regulate mood and emotional states effectively. The heightened reactivity of the subcortical brain, combined with the formation of strong associations, can result in mood dysregulation, anxiety, and even conditions like PTSD. Individuals who have experienced trauma may find it challenging to control their emotional responses to triggers, as these triggers are linked to overwhelming emotions stored in the subcortical brain.
Brainspotting’s Role in Memory and Association Modification:
Brainspotting, as a therapeutic approach, is thought to disrupt these maladaptive associations and help the brain reprocess traumatic memories in a more adaptive way. The therapy often involves identifying and processing brainspots—specific eye positions that correlate with emotional activation related to traumatic memories. By focusing on these spots and engaging in therapeutic processing, individuals may trigger intense emotional and somatic responses in the subcortical brain. This intense stimulation, in theory, forces the brain to confront and reprocess these associations and emotions. Over time, through repeated Brainspotting sessions, it’s believed that the brain may learn to hold and process these emotions differently and establish new, less distressing associations.
Delayed Emergence of Memories and Associations:
The delay in the emergence of memories and associations during Brainspotting processing can be attributed to the complexity of the brain’s processing mechanisms. While subcortical brain structures may be engaged and stimulated during therapy, it takes time for these changes to be integrated and for new associations to form. The midbrain and frontal cortex, responsible for higher-order processing, interpretation, and regulation of emotions, may need time to catch up to the changes that occurred at the subcortical level during therapy sessio
What are the measurable effects of Brainspotting:
Emotional Regulation:
Brainspotting can help individuals access and process deep-seated emotional content related to traumatic experiences. This emotional content often involves the limbic system, including structures like the amygdala (part of subcortical regions) that play a central role in emotional processing. By addressing and resolving emotional trauma, Brainspotting may contribute to more effective emotional regulation over time, potentially influencing the functioning of the limbic system.
Memory Processing:
Traumatic memories and emotions associated with them can be stored in various parts of the brain, including the hippocampus (a subcortical structure) involved in memory formation. Brainspotting aims to facilitate the processing and integration of these traumatic memories, potentially leading to a reduction in their emotional intensity and intrusive nature.
Self-Awareness and Self-Reflection:
Brainspotting involves a process of self-awareness and self-reflection, which may engage the precuneus and related brain regions involved in introspective thinking. As individuals engage in Brainspotting sessions and explore their emotional experiences and memories, they may enhance their self-awareness and self-understanding.
How does Brainspotting work in the Brain?
Brainspotting is a therapeutic technique that is thought to work by engaging various theoretical mechanisms of action in the brain. While research on this topic continues to evolve, here are some of the theoretical mechanisms associated with Brainspotting:
Limbic System Regulation:
Brainspotting may help regulate the limbic system, which is involved in processing emotions and memories. By identifying and processing “brainspots” (specific eye positions correlated with emotional activation), it is believed that this technique can access and modulate deep-seated emotional responses.
Dual-Attention:
Brainspotting involves maintaining dual attention, where the client simultaneously focuses on an external point (the brainspot) and their internal experience (thoughts, emotions, sensations). This dual attention may help desensitize traumatic memories and reduce their emotional charge.
Neurobiological Integration:
It’s theorized that Brainspotting can facilitate the integration of fragmented or dissociated neural networks related to traumatic experiences. By doing so, it may help individuals process and heal from past traumas.
Mirror Neurons:
Mirror neurons in the brain are thought to play a role in empathy and emotional regulation. Brainspotting might activate mirror neuron pathways, enhancing the therapeutic relationship and promoting emotional connection.
Brainwave Regulation:
Some suggest that Brainspotting may influence brainwave patterns, shifting from states of hyperarousal (e.g., anxiety) to more balanced and relaxed states. This can help clients achieve a calmer, more focused mental state.
Proprioceptive and Interoceptive Awareness:
Brainspotting may increase awareness of bodily sensations and emotions (interoception) and spatial orientation (proprioception). This heightened awareness can aid in processing and resolving emotional issues.
How Does Brainspotting and ETT use implicit memory?
Implicit memory, a type of long-term memory, is associated with different regions of the brain, including the frontal subregions and midbrain structures. Here are some mechanisms involving these brain areas and implicit memory:
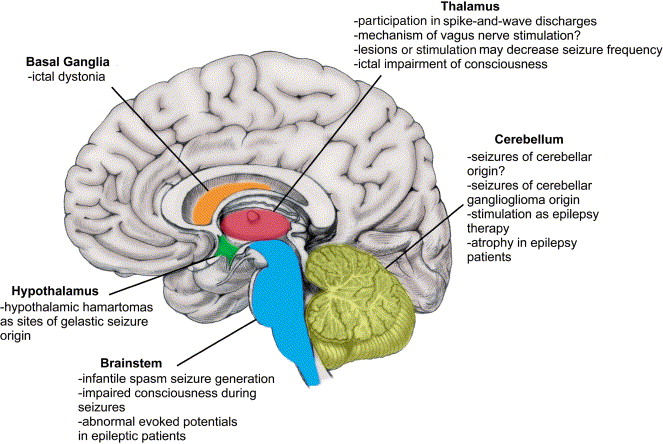
Basal Ganglia and Implicit Procedural Memory:
The basal ganglia, a group of structures within the midbrain, plays a crucial role in implicit procedural memory. This type of memory involves learning and remembering how to perform tasks or skills, such as riding a bike or typing. The basal ganglia helps consolidate and automate these motor and procedural skills over time.
Frontal Cortex and Habitual Learning:
The frontal cortex, particularly the dorsolateral prefrontal cortex (DLPFC), is involved in implicit memory related to habitual learning and behavioral priming. This brain region aids in the acquisition and execution of automatic and routine behaviors. For example, when you repeatedly perform a task or make decisions, the DLPFC becomes more efficient in guiding these actions.
Emotional Implicit Memory and Amygdala:
The amygdala, located within the midbrain, plays a significant role in implicit memory associated with emotions and emotional conditioning. Emotional experiences can become implicitly stored in memory, influencing future emotional responses. The amygdala helps to encode and retrieve these emotionally charged memories.
Cerebellum and Motor Skill Memory:
The cerebellum, located at the back of the brain, is crucial for implicit memory linked to motor skills and coordination. It stores and refines motor patterns, allowing for smoother and more precise movements. This is evident in activities like playing musical instruments or sports.
Implicit Memory Consolidation during Sleep:
While not specific to the frontal subregions or midbrain, implicit memories are known to undergo consolidation during sleep. The brain processes experiences and skills learned during the day, transferring them from short-term to long-term memory storage, which can involve various brain regions, including the hippocampus.
Neural Plasticity:
Implicit memory formation often relies on neural plasticity—the brain’s ability to adapt and reorganize its connections. Neuroplastic changes occur in response to repeated experiences or stimuli, leading to the strengthening of implicit memories in relevant brain regions.
Did you enjoy this article? Checkout the podcast here: https://gettherapybirmingham.podbean.com/
Bibliography:
Grand, D. (2013). Brainspotting: The Revolutionary New Therapy for Rapid and Effective Change. Sounds True.
Shapiro, F. (2017). Eye Movement Desensitization and Reprocessing (EMDR) Therapy, Third Edition: Basic Principles, Protocols, and Procedures. The Guilford Press.
Vazquez, S. R. (2009). Emotional Transformation Therapy: An Interactive Ecological Psychotherapy. Jason Aronson, Incorporated.
Bandler, R., & Grinder, J. (1979). Frogs into Princes: Neuro Linguistic Programming. Real People Press.
Beaulieu, D. (2003). Eye Movement Integration Therapy: The Comprehensive Clinical Guide. Crown House Publishing.
Rapaille, C. (2007). The Culture Code: An Ingenious Way to Understand Why People Around the World Live and Buy as They Do. Broadway Books.
Laeng, B., Sirois, S., & Gredebäck, G. (2012). Pupillometry: A Window to the Preconscious? Perspectives on Psychological Science, 7(1), 18-27.
Oka, S., Chapman, C. R., Kim, B., Nakajima, I., Shimizu, O., & Oi, Y. (2007). Pupil dilation response to noxious stimulation: effect of varying nitrous oxide concentration. Clinical Neurophysiology, 118(9), 2016-2024.
Laeng, B., & Sulutvedt, U. (2014). The Eye Pupil Adjusts to Imaginary Light. Psychological Science, 25(1), 188-197.
Further Reading:
Corrigan, F. M., & Grand, D. (2013). Brainspotting: Recruiting the midbrain for accessing and healing sensorimotor memories of traumatic activation. Medical Hypotheses, 80(6), 759-766.
Daniels, J. K., & McFarlane, A. C. (2019). Neurobiology of traumatic stress disorders and their impact on physical health. Dialogues in Clinical Neuroscience, 21(3), 255-273.
Einhäuser, W. (2017). The Pupil as Marker of Cognitive Processes. In Q. Zhao (Ed.), Computational and Cognitive Neuroscience of Vision (pp. 141-169). Springer Singapore.
Nummenmaa, L., Glerean, E., Hari, R., & Hietanen, J. K. (2014). Bodily maps of emotions. Proceedings of the National Academy of Sciences, 111(2), 646-651.
Porges, S. W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W. W. Norton & Company.
Schwartz, M. S., Andrasik, F., & Andrasik, F. (Eds.). (2017). Biofeedback: A Practitioner’s Guide. The Guilford Press.
van der Kolk, B. (2015). The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma. Penguin Books.










0 Comments