
The Architect of Personality: Beyond the Stigma of Borderline
Borderline Personality Disorder (BPD) is perhaps the most stigmatized and misunderstood diagnosis in the Diagnostic and Statistical Manual of Mental Disorders (DSM). Often dismissed as “manipulative” or “untreatable,” BPD is better understood as a complex trauma response—a frantic attempt to regulate a nervous system that was never taught how to soothe itself. While modern psychiatry often focuses on symptom management, the work of Theodore Millon offers a deeper, evolutionary understanding of the disorder.
Millon did not view BPD as a random collection of symptoms but as a structural personality style that developed to survive a chaotic environment. His work bridges the gap between the biological reality of the brain and the biographical reality of the patient. By understanding Millon’s subtypes, we can move beyond the label and treat the unique human being underneath.
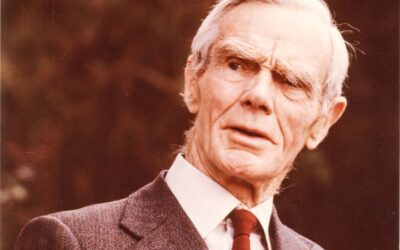
Who Was Theodore Millon?
Theodore Millon (1928–2014) was a giant in the field of personality theory. Unlike many of his contemporaries who were strictly clinicians, Millon was a true polymath—integrating evolutionary biology, physics, and philosophy into his psychological models. He famously argued that a diagnosis without a theory is just a list of complaints. He believed we needed to understand the function of a personality style before we could treat it.
He is best remembered as the primary force behind the personality disorder sections of the DSM-III (1980) and DSM-IV (1994). He championed the “Multiaxial System” (Axis II), which ensured that personality disorders were given equal weight to acute conditions like depression. This was a revolutionary shift that forced the medical community to look at the whole person, not just their current mood.
A Critic of the DSM-5
Millon was not involved in the creation of the DSM-5; rather, he was one of its fiercest critics. He argued that the DSM-5’s move toward a purely biological and trait-based model stripped away the narrative nuance of the human experience. He believed that reducing personality to a set of statistical traits ignored the evolutionary purpose of those behaviors. He died in January 2014, shortly after the publication of the DSM-5, having spent his final years warning against the over-medicalization of personality.
Timeline of Theodore Millon’s Contributions
| Year | Event / Publication |
| 1928 | Born in New York City. |
| 1969 | Publishes Modern Psychopathology, introducing his biosocial learning theory. |
| 1980 | Serves as a key member of the DSM-III Task Force, establishing the Multiaxial System. |
| 1996 | Publishes Disorders of Personality: DSM-IV and Beyond, detailing the BPD subtypes. |
| 2013 | DSM-5 is published; Millon criticizes its removal of the multiaxial system. |
| 2014 | Dies in Greenville, SC. |
The Four Faces of Borderline Personality
One of Millon’s most enduring contributions is his subtyping of Borderline Personality Disorder. He recognized that two people with BPD can look completely different. One might be quiet and withdrawn, while the other is explosive and reckless. Understanding these “flavors” is crucial for effective treatment planning, whether using Internal Family Systems or DBT.
1. The Discouraged Borderline
This subtype leans heavily towards the avoidant and depressive spectrum. These individuals are not “acting out” but “acting in.” They are often compliant, submissive, and “clingy”—not out of entitlement, but out of a profound sense of helplessness. They feel they have no right to exist independently and often merge with others to feel safe.
Key Feature: “I am nothing without you.”
Trauma Origin: Often associated with emotional neglect where the child learned that having needs was dangerous.
2. The Impulsive Borderline
Here, the instability is externalized. These individuals are often charismatic, energetic, and flirtatious, but prone to sudden, catastrophic loss of control. They seek external stimulation—sex, drugs, spending, gambling—to drown out an internal sense of emptiness or doom.
Key Feature: “I need to feel something, anything, right now.”
Trauma Origin: Can be linked to chaotic households where inconsistent rewards led to a dysregulated dopamine system. This aligns with the neurobiology of shame and the need for immediate regulation.
3. The Petulant Borderline
Characterized by negativity, impatience, and defiance. They often feel wronged by the world and demand restitution. They test relationships by pushing people away, only to feel validated when the person leaves (“I knew you didn’t love me”). This is a defense mechanism: “I will reject you before you can reject me.”
Key Feature: “You owe me this because you hurt me.”
Trauma Origin: Similar to the “moving against” type described by Karen Horney, this is a fight response to feeling unprotected.
4. The Self-Destructive Borderline
The most tragic subtype, these individuals turn their rage inward. They are often high-functioning and conforming on the surface but harbor intense self-hatred. They may punish themselves for having needs or feelings. Self-harm here is not a “cry for help” but a way to execute the self for imagined crimes.
Key Feature: “I am bad and I deserve to suffer.”
Trauma Origin: High risk of self-harm and suicidality. This behavior is often a “safety valve” to prevent the expression of rage toward a loved object (parent/partner), protecting the relationship at the cost of the self.
The Conceptualization of Trauma: Structural Deformity vs. Disease
Millon’s greatest contribution was reframing personality disorders not as “sicknesses” (like a virus you catch) but as failed adaptations. He viewed the personality as the psychological immune system. In BPD, this immune system is hyperactive—attacking the self and others to ward off the threat of abandonment.
The “Cluster B” Removal Controversy
Millon was a staunch defender of the “Cluster” system in the DSM (grouping Dramatic/Erratic disorders together). He believed that BPD, Narcissism, and Histrionic disorder were genetically and traumatically linked—often different outcomes of the same chaotic childhood environment.
The Modern Shift: The removal of the Multiaxial system in the DSM-5 moves psychiatry toward a flatter, more biological model. While scientifically interesting, this shift risks losing the narrative of the patient. Millon’s subtypes help patients understand why they act the way they do, which is the first step in healing from narcissistic abuse and trauma.
Conclusion: The Legacy of Complexity
Theodore Millon taught us that diagnosis is not a stamp of doom but a map of the territory. His work bridges the gap between the neuroscience of trauma and the humanistic understanding of suffering. By identifying the specific subtype of BPD, therapists can move beyond generic “coping skills” and address the core structural wound of the patient.
Whether using Dialectical Behavior Therapy (DBT) or psychodynamic approaches, Millon’s taxonomy remains a vital tool for clinicians helping clients navigate the stormy waters of the borderline experience.
Bibliography
- Millon, T. (2011). Disorders of Personality: Introducing a DSM/ICD Spectrum from Normal to Abnormal. Wiley.
- Millon, T., & Davis, R. D. (1996). Disorders of Personality: DSM-IV and Beyond. Wiley.
- Strack, S., & Millon, T. (Eds.). (2007). Handbook of Personology and Psychopathology. Wiley.
- American Psychiatric Association. (1980). Diagnostic and Statistical Manual of Mental Disorders (3rd ed.).
- Huprich, S. K. (2014). “Theodore Millon (1928–2014).” American Psychologist, 69(5), 552.














0 Comments