
Key Takeaways: Physician Burnout & Moral Injury
- Prevalence: Over 50% of physicians report symptoms of burnout, making it a public health crisis affecting patient safety.
- Key Distinction: “Burnout” implies a lack of resilience; Moral Injury describes the distress of being forced to violate ethical values by a broken healthcare system.
- Neurobiology: Chronic stress shrinks the prefrontal cortex (decision making) and enlarges the amygdala (fear center), leading to depersonalization.
- Treatment: Requires a dual approach of systemic change (reducing administrative load) and individual somatic therapy (Brainspotting, Neurofeedback) to reset the nervous system.
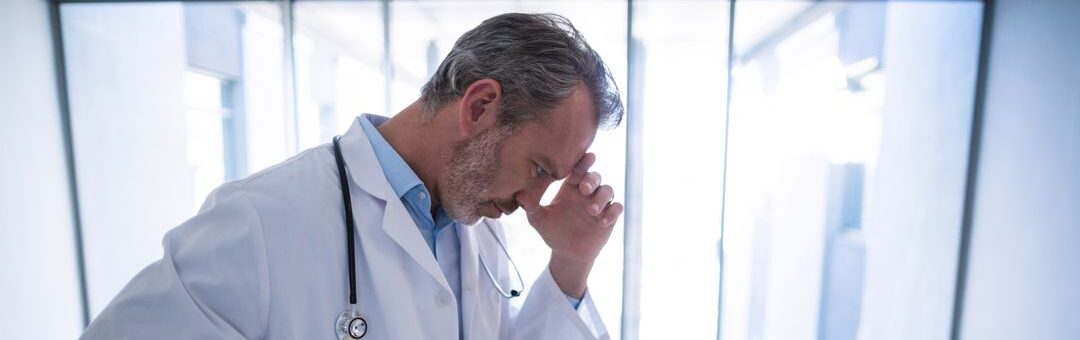
Physician burnout has become the defining crisis of modern healthcare. It is not merely “job dissatisfaction”; it is a syndrome characterized by emotional exhaustion, depersonalization (cynicism), and a decreased sense of personal accomplishment. Studies consistently show that over 50% of physicians experience at least one symptom of burnout.
This is a silent epidemic with loud consequences. When a doctor burns out, it is not just a personal tragedy; it is a public safety hazard. The cognitive impairment associated with burnout correlates directly with increased medical errors, lower patient satisfaction, and a mass exodus from the profession. To treat it, we must stop viewing it solely as a failure of individual resilience and start recognizing it as a symptom of a system in distress.
We Have a Clinician who Treats Physician Burnout at Taproot Therapy Collective – Check Him Out Here
Part 1: The Diagnosis – Burnout vs. Moral Injury
For years, the term “burnout” has been the standard diagnosis. However, many clinicians argue this term is victim-blaming. It suggests the physician simply “ran out of fuel.” A more accurate framework for many is Moral Injury.
| Feature | Burnout | Moral Injury |
| Primary Cause | Excessive workload, lack of sleep, bureaucratic drudgery. | Being forced to act against one’s ethical code (e.g., denying care due to insurance, rushing patients). |
| Internal Experience | Exhaustion, “I can’t do this anymore.” | Guilt, shame, anger, “I am betraying my oath.” |
| Systemic Role | System demands too much energy. | System demands a violation of values. |
Part 2: The Multi-Faceted Causes of Burnout
The causes of physician burnout are a complex web of systemic pressures and psychological traits.
1. The “EHR” Effect and Administrative Burden
The introduction of Electronic Health Records (EHRs) was meant to streamline care. Instead, it turned doctors into data entry clerks. Studies show that for every hour of patient care, physicians spend two hours on paperwork. This “pajama time”—charting late into the night—erodes the recovery time necessary for cognitive maintenance.
2. Loss of Autonomy
Physicians often feel like cogs in a corporate machine. The shift from private practice to hospital employment means doctors have less control over their schedules, patient volume, and clinical decisions. This loss of agency is a primary driver of psychological distress.
3. The “Invincibility” Myth
Medical culture valorizes self-sacrifice. From residency onwards, doctors are trained to suppress biological needs (sleep, hunger, emotion). This creates a psychological split: the “Iron Doctor” persona versus the vulnerable human being. Maintaining this split requires immense psychic energy.
Part 3: The Neuroscience of the Burned-Out Brain
Burnout is not just “in your head”; it is a physical alteration of the brain structure.
- Amygdala Hijack: Chronic stress enlarges the amygdala (the brain’s threat detection center), keeping the physician in a constant state of “fight or flight.”
- Prefrontal Cortex Atrophy: The area responsible for complex decision-making and empathy thins under chronic stress. This explains why burned-out doctors struggle with complex diagnoses and feel emotionally numb.
- Depersonalization as Defense: To protect itself from the pain of empathy, the brain disconnects. Patients become “objects” or “tasks.” This is a survival mechanism, but it destroys the therapeutic alliance.
Part 4: The Severe Consequences
For the Patient: Safety Risks
A burned-out brain is an impaired brain. Evidence links burnout to a significant increase in medical errors. When attention is fractured by exhaustion, details are missed. Furthermore, the depersonalization aspect leads to poor communication, which is a leading cause of malpractice suits.
For the Physician: The Suicide Crisis
Physicians have the highest suicide rate of any profession—more than twice that of the general population. The combination of easy access to lethal means, high knowledge of anatomy, and extreme stigma against seeking mental health care creates a deadly storm.
Part 5: Treatment and Recovery Strategies
Recovering from burnout requires moving beyond “resilience training” (which can feel like gaslighting) toward deep structural and psychological change.
1. Somatic and Neurological Therapies
Because burnout changes the brain, “talk therapy” isn’t always enough. We need to reset the nervous system.
* Neurofeedback: Can train the brain out of the high-beta “stress” waves and back into a regulated state.
* Brainspotting: Allows physicians to process the visual trauma of their work (codes, injuries) without having to verbally relive it.
* Somatic Experiencing: Helps discharge the “freeze” response accumulated after years of suppressing emotion in high-stakes environments.
2. Addressing the “Shadow”
In Jungian Therapy, we work with the physician’s “Shadow”—the parts of themselves they had to repress to become a doctor (creativity, rest, vulnerability). Integrating these lost parts is essential for feeling whole again.
3. Systemic Boundaries
Therapy also involves coaching on how to navigate the system. This might mean setting hard boundaries on work hours, negotiating administrative support, or recognizing when a toxic work environment is essentially abusive and planning an exit.
Part 6: Prevention in Medical Education
The cure must begin upstream. Medical schools are starting to address the “Hidden Curriculum”—the unspoken norms that teach students to devalue their own well-being. By incorporating mindfulness, normalizing mental health care, and teaching the realities of moral injury, we can inoculate the next generation of healers against this plague.
Conclusion
Physician burnout is a systemic failure, not a personal weakness. However, recovery often begins with the individual act of seeking help. By utilizing advanced therapies and reframing the experience from “failure” to “injury,” physicians can reclaim their lives and their passion for medicine.
Book a Confidential Consultation for Physician Burnout
Explore Depth Psychology & Professional Mental Health
Taproot Therapy Collective Podcast
Trauma & Recovery Modalities
- Brainspotting: Processing trauma through the visual field.
- QEEG Brain Mapping: Visualizing the burned-out brain.
- Somatic Experiencing: Releasing stored stress from the body.
- EMDR: Desensitizing traumatic medical memories.
- Somatic Trauma Mapping: Locating stress in the body.
Psychological Frameworks
- Personality Psychology: Traits of the medical professional.
- Lifespan Integration: Reconnecting with the pre-medical self.
- DBT: Skills for distress tolerance in high-stakes environments.
- DARVO: Recognizing institutional gaslighting.
Bibliography
- Shanafelt, T. D., et al. (2021). Changes in Burnout and Satisfaction With Work-Life Integration in Physicians During the First 2 Years of the COVID-19 Pandemic. Mayo Clinic Proceedings.
- Dean, W., & Talbot, S. G. (2018). Physicians aren’t ‘burning out.’ They’re suffering from moral injury. STAT News.
- West, C. P., Dyrbye, L. N., & Shanafelt, T. D. (2016). Physician burnout: contributors, consequences and solutions. The Lancet.
- Dutheil, F., et al. (2021). PTSD as the second tsunami of the SARS-CoV-2 pandemic. Psychological Medicine.
- Arnsten, A. F. (2009). Stress signalling pathways that impair prefrontal cortex structure and function. Nature Reviews Neuroscience.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. If you are a physician experiencing suicidal thoughts, please contact the National Suicide Prevention Lifeline or the Physician Support Line immediately.













0 Comments