
Understanding Dissociation, DID, and Complex Trauma
An interactive clinical guide and self-screener exploring the spectrum of dissociation, the intersection of neurodivergence, and the modern, evidence-based guidelines for treating Structural Dissociation.
The clinical landscape regarding trauma and dissociation has radically evolved. We now understand that dissociation is not a sign of "brokenness," but rather the nervous system's ultimate, brilliant survival strategy. When a developing child cannot physically escape an abusive or severely neglectful environment, the mind escapes the body. It compartmentalizes the unbearable agony into separate ego-states so that the child can continue to function in daily life.
At Taproot Therapy Collective, we recognize that what begins as a lifesaving neurobiological adaptation in childhood often becomes a profoundly distressing reality in adulthood. We invite you to explore the interactive guide below to learn about the clinical criteria of Dissociative Identity Disorder (DID), reflect on your own experiences using the screener, and understand how conditions like Autism and ADHD can frequently overlap with or mimic dissociative symptoms.
Welcome to the Interactive GuideFeeling disconnected is a universal human experience. We all "zone out" on a long drive, get lost in a good book, or daydream. This is a mild, everyday form of dissociation.
For some, however, this sense of disconnection is severe, persistent, and deeply distressing, fragmenting their very sense of self, their memories, and their perception of the world. This experience is the hallmark of dissociative disorders, the most complex of which is Dissociative Identity Disorder (DID).
This application is an educational guide and self-reflection tool. It provides information on DID, an informal screener to help you reflect on your own experiences, and resources for further help. It is not a substitute for a professional diagnosis.
Clinical Best Practices: Why Standard Interventions Fail DID
If you or a loved one identify with the structural dissociation outlined in the screener above, it is imperative to understand that standard trauma interventions can be actively dangerous if applied incorrectly. The nervous system of an individual with DID has erected massive amnesiac barriers precisely to prevent the conscious mind from being flooded by unbearable, overwhelming traumatic memory.
The ISSTD Phase-Oriented Treatment Model
According to the International Society for the Study of Trauma and Dissociation (ISSTD), treatment for DID must strictly adhere to a three-phase model. Applying rapid exposure therapy or standard EMDR without immense preparation can violently collapse the patient's internal barriers, resulting in catastrophic psychological flooding, self-harm, or rapid hospitalization.
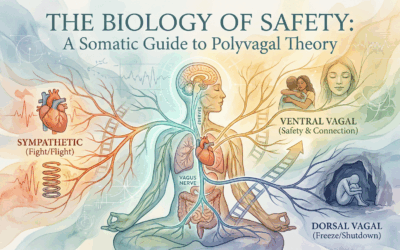
- Phase 1: Safety, Stabilization, and Symptom Reduction. This phase can last years. The clinical priority is establishing absolute environmental and bodily safety. Utilizing Somatic Experiencing and grounding techniques, the therapist helps the patient expand their "window of tolerance."
- Phase 2: Working with Traumatic Memory. Only once the patient's internal "parts" have established co-consciousness and a foundation of safety can the therapist begin to gently titrate the processing of traumatic memories using heavily modified, advanced protocols.
- Phase 3: Integration and Rehabilitation. The final phase involves integrating the fragmented identities into a cohesive, singular sense of self (or achieving healthy, cooperative functioning among parts) and learning to live a full life devoid of chronic defensive responses.
Modifying EMDR for Structural Dissociation
While Eye Movement Desensitization and Reprocessing (EMDR) is a highly effective, empirically validated treatment for single-event PTSD, standard EMDR is absolutely contraindicated for DID. Rapid bilateral stimulation forces the brain's neural networks to connect; in a patient with DID, this can accidentally force an unprepared host personality to collide instantly with the agonizing memories held by an exiled trauma part.
At Taproot Therapy Collective, our specialized trauma clinicians integrate EMDR with Parts-Based Therapy (Internal Family Systems) and Brainspotting. We never utilize rapid bilateral eye movements early in treatment. Instead, we use slow, carefully paced, externally focused interventions to help the different parts of the personality establish trust with the therapist before any deep subcortical processing is permitted.
Our Clinical Specialists
Treating complex, structural dissociation demands advanced post-graduate certification and a fierce commitment to pacing and safety. Review the credentials of our clinicians delivering neuro-somatic care to the Greater Birmingham area:
Find Safety Within Your Own Nervous System
Dissociation is not a sign of brokenness; it is the mind's ultimate survival strategy. You do not have to carry the weight of fragmentation forever. Partner with clinicians trained to safely navigate the complexities of your internal architecture.
Schedule a Clinical Assessment
















0 Comments