
What is Every Model of Therapy and Why Do They All Exist?
Psychotherapy is a vast field with numerous approaches, techniques, and models developed over decades of research and practice. This comprehensive dictionary aims to demystify the various types of psychotherapy, providing insights into their founders, approaches, techniques, focus, historical context, and criticisms. Whether you’re a mental health professional, student, or simply curious about the world of psychotherapy, this guide will help you navigate the diverse landscape of therapeutic approaches.
Timeline of the Development of all Models of Therapy
Complete List of Every Psychotherapy Modality.
Accelerated Experiential Dynamic Psychotherapy (AEDP)
Founder: Diana Fosha
Approach: AEDP integrates attachment theory, affective neuroscience, body-focused approaches, and transformational studies.
Techniques:
- Moment-to-moment tracking of emotional experience
- Dyadic affect regulation
- Meta-therapeutic processing
Focus: AEDP focuses on healing emotional suffering and fostering resilience by helping clients process difficult emotions and experiences.
Historical Context: AEDP emerged in the late 1990s as a response to traditional psychodynamic approaches that were seen as too slow or ineffective for some clients.
Criticisms:
- Some critics argue that the approach may be too intense for certain clients.
- There is a need for more empirical research to support its effectiveness.
Accelerated Resolution Therapy (ART)
Founder: Laney Rosenzweig
Techniques:
- Voluntary memory/image replacement
- Horizontal eye movements
- Metaphors and rescripting
Focus: ART aims to quickly resolve symptoms of trauma and other mental health problems by reprogramming the way distressing memories and images are stored in the brain.
Historical Context: ART was developed in 2008 as a faster alternative to traditional trauma therapies.
Criticisms:
- Some question the rapidity of change claimed by ART practitioners.
- More research is needed to establish its long-term effectiveness compared to other trauma therapies.
Attachment-Based Family Therapy (ABFT)
Founders: Guy Diamond, Gary Diamond, and Suzanne Levy
Techniques:
- Relational reframes
- Alliance building
- Attachment-promoting tasks
- Emotion-focused interventions
Focus: The focus is on strengthening family relationships and improving communication to create a secure base for adolescent development.
Historical Context: ABFT was developed in the 1990s, integrating attachment theory with structural and emotion-focused family therapy approaches.
Criticisms:
- Some question whether the approach is equally effective for all types of family structures and cultural backgrounds.
- There is ongoing research to establish its effectiveness compared to other family therapy approaches.
Brainspotting
Founder: David Grand
Techniques:
- Identifying and maintaining relevant eye positions
- Focused mindfulness
- Body scanning
- Bilateral sound (optional)
Focus: The focus is on locating, processing, and releasing sources of trauma and distress in the body and nervous system.
Historical Context: Brainspotting was discovered in 2003 by David Grand, evolving from his work with EMDR.
Criticisms:
- Some question the theoretical basis for the connection between eye positions and trauma processing.
- More research is needed to establish its effectiveness compared to other trauma therapies.
Clean Language and Symbolic Modeling
Founders: David Grove (Clean Language), Penny Tompkins and James Lawley (Symbolic Modeling)
Techniques:
- Clean questions
- Developing client-generated metaphors
- Spatial arrangement of symbols
- Identifying patterns and relationships in the client’s symbolic world
Focus: The focus is on helping clients gain insight and create change by exploring their own unique mental models and metaphors.
Historical Context: Clean Language was developed by David Grove in the 1980s, with Symbolic Modeling further developed by Tompkins and Lawley in the 1990s.
Criticisms:
- Some argue that the approach may be too abstract or indirect for clients seeking more concrete interventions.
- There is limited empirical research on its effectiveness compared to other therapeutic approaches.
Coherence Therapy
Founders: Bruce Ecker and Laurel Hulley
Techniques:
- Symptom deprivation
- Retrieval of pro-symptom positions
- Juxtaposition experiences
- Memory reconsolidation
Focus: The focus is on facilitating transformational change by bringing unconscious, symptom-generating schemas into conscious awareness and creating experiences that contradict these schemas.
Historical Context: Coherence Therapy was developed in the 1990s, drawing on neuroscience research about memory reconsolidation and integrating elements from various psychotherapy approaches.
Criticisms:
- Some question whether the rapid changes claimed by Coherence Therapy are sustainable long-term.
- There is a need for more empirical research to support its effectiveness across different populations and conditions.
Developmental Model of Couples Therapy
Founders: Ellyn Bader and Peter Pearson
Techniques:
- Developmental assessment
- Differentiation exercises
- Attachment-based interventions
- Addressing symbiosis and projective identification
Focus: The focus is on helping couples progress through developmental stages, balancing individual growth with couple intimacy.
Historical Context: The Developmental Model was created in the 1980s, integrating concepts from attachment theory, differentiation theory, and neuroscience.
Criticisms:
- Some argue that the model may not adequately address cultural differences in relationship development.
- Critics question whether all relationships follow the proposed developmental stages.
Discernment Counseling
Founder: William J. Doherty
Techniques:
- Individual and couple sessions
- Exploration of relationship history
- Clarification of individual and couple goals
- Decision-making support
Focus: The focus is on helping couples make a clear and confident decision about the future of their relationship, whether that involves reconciliation or divorce.
Historical Context: Discernment Counseling was developed in the 2000s as a response to the limitations of traditional couples therapy for “mixed-agenda” couples.
Criticisms:
- Some argue that the short-term nature of the intervention may not be sufficient for complex relationship issues.
- Critics question whether the approach can truly remain neutral in the face of divergent partner goals.
Emotional Transformation Therapy (ETT)
Founder: Steven Vazquez
Techniques:
- Visual brain stimulation
- Color therapy
- Eye movement techniques
- Rapid emotional processing
Focus: The focus is on quickly accessing and transforming underlying emotional states that contribute to psychological problems.
Historical Context: ETT was developed in the 1990s, integrating concepts from neuroscience, color psychology, and various psychotherapeutic approaches.
Criticisms:
- Some question the scientific basis for the use of light and color in psychological treatment.
- There is limited empirical research on its effectiveness compared to established therapies.
Encounter-Centered Couples Therapy
Founders: Hedy Schleifer and Yumi Schleifer
Techniques:
- Crossing the bridge (structured dialogue)
- Relational space creation
- Embracing the “three invisible connectors” (the space, the bridge, the encounter)
- Somatic awareness exercises
Focus: The focus is on helping couples move beyond surface conflicts to create profound emotional and spiritual connections.
Historical Context: Encounter-Centered Couples Therapy was developed in the 2000s, drawing on various relational and experiential approaches.
Criticisms:
- Some argue that the approach may be too intense or spiritually oriented for some couples.
- Critics question whether the structured nature of the encounters can translate to everyday interactions.
Existential Analysis
Founder: Alfried Längle (building on the work of Viktor Frankl)
Techniques:
- Phenomenological analysis
- Dialogue on existential themes
- Value clarification
- Decision-making processes
Focus: The focus is on enhancing a person’s ability to live with inner consent, make authentic decisions, and engage meaningfully with the world.
Historical Context: Existential Analysis developed from the 1980s onward as an extension and elaboration of Viktor Frankl’s logotherapy.
Criticisms:
- Some argue that the approach may be too philosophical or abstract for clients seeking more concrete interventions.
- Critics question whether focusing on existential themes is appropriate for all types of psychological issues.
Focusing-Oriented Art Therapy
Founder: Laury Rappaport
Techniques:
- Felt sense exploration through art
- Clearing a space with art materials
- Symbolic representation of inner experiences
- Dialogue with artwork
Focus: The focus is on using art to access, explore, and express the bodily felt sense of issues or situations.
Historical Context: Focusing-Oriented Art Therapy was developed in the 1990s, combining Gendlin’s Focusing with established art therapy practices.
Criticisms:
- Some question whether the combination of Focusing and art therapy offers significant advantages over either approach alone.
- Critics argue that the approach may be challenging for clients who are uncomfortable with either Focusing or artistic expression.
Formative Psychology
Founder: Stanley Keleman
Techniques:
- Voluntary muscular-cortical effort
- Anatomical education
- Somatic exercises
- Exploring personal history through bodily patterns
Focus: The focus is on helping individuals understand and influence their own formative process to create new behavioral and emotional possibilities.
Historical Context: Formative Psychology was developed by Stanley Keleman from the 1970s onwards, building on his background in bioenergetics and his own theoretical formulations.
Criticisms:
- Some argue that the approach’s emphasis on bodily structure may oversimplify complex psychological issues.
- There is limited empirical research on its effectiveness compared to other somatic or psychological approaches.
Functional Analytic Psychotherapy (FAP)
Founders: Robert Kohlenberg and Mavis Tsai
Techniques:
- Identifying clinically relevant behaviors
- Natural reinforcement of adaptive behaviors
- Functional analysis of in-session behaviors
- Therapeutic use of self-disclosure
Focus: The focus is on creating intense, genuine relationships in therapy to evoke and reinforce adaptive behaviors that can generalize to clients’ daily lives.
Historical Context: FAP was developed in the 1990s as part of the third wave of behavioral therapies, emphasizing contextualism and the therapeutic relationship.
Criticisms:
- Some argue that the intense focus on the therapeutic relationship may blur professional boundaries.
- Critics question whether changes in in-session behaviors reliably translate to real-world improvements.
Holographic Memory Resolution (HMR)
Founder: Brent Baum
Techniques:
- Somatic awareness
- Color-coding of emotional states
- Accessing and resolving “sensory capsules”
- Integration of resolved trauma memories
Focus: The focus is on accessing and transforming traumatic memories stored in the body, without the need for extensive verbal processing or re-experiencing of trauma.
Historical Context: HMR was developed in the 1980s and 1990s, drawing on concepts from holography, neuroscience, and somatic therapies.
Criticisms:
- Some question the scientific basis for the concept of “holographic” memory storage in the body.
- There is limited empirical research on its effectiveness compared to established trauma therapies.
Identity-Oriented Psychotrauma Therapy (IoPT)
Founder: Franz Ruppert
Techniques:
- Intention method
- Trauma constellations
- Exploring multigenerational trauma patterns
- Integration of split parts of the psyche
Focus: The focus is on identifying and resolving the impacts of early trauma on identity formation and current psychological functioning.
Historical Context: IoPT was developed by Franz Ruppert in the early 2000s, building on family constellation work and trauma theory.
Criticisms:
- Some argue that the approach may oversimplify complex psychological and systemic issues.
- Critics question the empirical basis for some of the theoretical concepts used in IoPT.
Internal Attachment Therapy
Founders: Dafna Lender and Denise Hughey
Techniques:
- Internal dialogue with attachment figures
- Reparenting exercises
- Somatic awareness of attachment needs
- Integration of fragmented self-states
Focus: The focus is on healing attachment wounds by creating secure internal attachments and integrating disowned parts of the self.
Historical Context: Internal Attachment Therapy was developed in the 2010s, integrating concepts from attachment theory, internal family systems, and somatic therapies.
Criticisms:
- Some question whether internal representations can effectively substitute for real-life secure attachments.
- There is limited empirical research on its effectiveness compared to other attachment-based therapies.
Intensive Short-Term Dynamic Psychotherapy (ISTDP)
Founder: Habib Davanloo
Techniques:
- Pressure to feel
- Challenge to defenses
- Head-on collision with resistance
- Unlocking of the unconscious
Focus: The focus is on rapidly breaking through psychological defenses to access and resolve core emotional conflicts.
Historical Context: ISTDP was developed by Habib Davanloo in the 1960s and 1970s, building on psychoanalytic principles but aiming for more rapid and intensive intervention.
Criticisms:
- Some argue that the approach may be too confrontational or intense for many clients.
- Critics question whether the rapid pace of therapy allows for sufficient processing and integration of emotional experiences.
Interpersonal Reconstructive Therapy (IRT)
Founder: Lorna Smith Benjamin
Techniques:
- Copy process analysis
- Gift of love intervention
- Collaborative case formulation
- Interpersonal pattern recognition and modification
Focus: The focus is on identifying and modifying internalized representations of early attachment figures that continue to influence current relationships and behaviors.
Historical Context: IRT was developed by Lorna Smith Benjamin in the 1970s and 1980s, integrating concepts from attachment theory, interpersonal theory, and learning theory.
Criticisms:
- Some argue that the approach may place too much emphasis on early relationships at the expense of current environmental factors.
- There is ongoing research to establish its effectiveness compared to other integrative therapies.
Lifespan Integration
Founder: Peggy Pace
Techniques:
- Time line repetitions
- Imaginal nurturing of younger self
- Body-mind integration
- Affect bridge
Focus: The focus is on integrating memories and experiences across the lifespan to create a more coherent sense of self and resolve long-standing issues.
Historical Context: Lifespan Integration was developed in the early 2000s, drawing on neuroscience research about memory reconsolidation and neural integration.
Criticisms:
- Some question the theoretical basis for the time line technique and its purported effects on neural integration.
- More research is needed to establish its effectiveness compared to other trauma-focused therapies.
Method of Levels (MOL)
Founder: Timothy A. Carey (based on William T. Powers’ Perceptual Control Theory)
Techniques:
- Open-ended questioning
- Following the client’s train of thought
- Attending to disruptions in thought flow
- Encouraging metaperception
Focus: The focus is on helping clients resolve internal conflicts by accessing higher-level goals and reorganizing their control systems.
Historical Context: MOL was developed in the early 2000s as an application of Perceptual Control Theory to psychotherapy.
Criticisms:
- Some argue that the approach may be too non-directive for clients seeking more structured interventions.
- There is limited empirical research on its effectiveness compared to other cognitive therapies.
Mindfulness-Based Relationship Enhancement
Founders: James W. Carson, Karen M. Gil, and Donald H. Baucom
Techniques:
- Partner-focused loving-kindness meditation
- Mindful touch exercises
- Acceptance practices for partner attributes
- Mindfulness in daily couple activities
Focus: The focus is on cultivating mindfulness skills to enhance relationship satisfaction, intimacy, and individual well-being within the context of romantic relationships.
Historical Context: Mindfulness-Based Relationship Enhancement was developed in the early 2000s, adapting mindfulness-based stress reduction for couples.
Criticisms:
- Some question whether mindfulness practices are equally beneficial for all types of relationship issues.
- Critics argue that the approach may not adequately address deep-seated relationship conflicts or incompatibilities.
Narrative Exposure Therapy (NET)
Founders: Maggie Schauer, Frank Neuner, and Thomas Elbert
Techniques:
- Chronological narration of life events
- Exposure to traumatic memories
- Contextualizing traumatic experiences
- Creating a coherent narrative
Focus: The focus is on reducing symptoms of PTSD by contextualizing traumatic experiences within the individual’s life story.
Historical Context: NET was developed in the early 2000s to address the needs of individuals who have experienced multiple traumatic events, particularly in conflict zones.
Criticisms:
- Some argue that the approach may be too intense for certain trauma survivors.
- Critics question whether the short-term nature of the treatment is sufficient for complex trauma cases.
Neuro-Affective Relational Model (NARM)
Founder: Laurence Heller
Techniques:
- Tracking nervous system responses
- Exploring identity distortions
- Working with core life themes
- Supporting nervous system regulation
Focus: The focus is on helping clients connect to their authentic self by resolving survival styles that developed due to developmental trauma.
Historical Context: NARM was developed in the 2000s, integrating elements from somatic therapies, attachment theory, and developmental psychology.
Criticisms:
- Some question whether the model’s focus on developmental trauma is relevant for all clients.
- There is ongoing research to establish its effectiveness compared to other trauma-informed approaches.
Observed & Experiential Integration (OEI)
Founders: Audrey Cook and Rick Bradshaw
Techniques:
- Switching visual attention between eyes
- Glitch removal (processing micro-traumas)
- Integration of dissociated aspects of trauma
- Titrated exposure to traumatic memories
Focus: The focus is on integrating dissociated aspects of traumatic experiences and resolving trauma-related symptoms through sensory-motor interventions.
Historical Context: OEI was developed in the 1990s, drawing on elements from EMDR and other trauma therapies.
Criticisms:
- Some argue that the approach lacks a strong theoretical foundation.
- There is limited empirical research on its effectiveness compared to established trauma therapies.
Panic-Focused Psychodynamic Psychotherapy (PFPP)
Founders: Barbara Milrod and colleagues
Techniques:
- Exploring unconscious meanings of panic symptoms
- Addressing separation anxiety and autonomy issues
- Analyzing transference in relation to panic
- Working through termination as it relates to panic
Focus: The focus is on understanding and resolving unconscious conflicts believed to underlie panic symptoms.
Historical Context: PFPP was developed in the 1990s to provide a psychodynamic alternative to cognitive-behavioral treatments for panic disorder.
Criticisms:
- Some question whether a psychodynamic approach is necessary or effective for a disorder often treated successfully with CBT.
- Critics argue that the short-term nature of the therapy may not be sufficient for exploring deep-seated conflicts.
Positive Psychotherapy (PPT)
Founders: Nossrat Peseschkian and colleagues
Techniques:
- Balance model analysis
- Positive interpretation
- Five-stage approach to conflict resolution
- Transcultural storytelling
Focus: The focus is on helping clients achieve a balance between various life domains and cultivate positive capacities.
Historical Context: PPT was developed in the 1960s and 1970s, integrating Eastern and Western concepts of psychology and philosophy.
Criticisms:
- Some argue that the approach may oversimplify complex psychological issues by focusing primarily on positives.
- Critics question whether the transcultural aspects of the therapy are equally applicable across all cultures.
Process-Oriented Psychology (Process Work)
Techniques:
- Amplification of subtle signals
- Unfolding of secondary processes
- Dreamwork and body symptom work
- Exploration of interpersonal and social fields
Focus: The focus is on following and amplifying subtle, often unconscious processes to bring them into awareness and integration.
Historical Context: Process Work was developed in the 1970s and 1980s, evolving from Jungian psychology and incorporating influences from physics, Taoism, and indigenous practices.
Criticisms:
- Some argue that the approach is too esoteric or abstract for many clients.
- Critics question the scientific basis for some of the concepts used in Process Work.
Psychobiological Approach to Couple Therapy (PACT)
Founder: Stan Tatkin
Techniques:
- Staging interactions to reveal implicit memories and expectations
- Cross-modal sensory awareness exercises
- Psychoeducation about neurobiology of relationships
- Moment-to-moment tracking of arousal states
Focus: The focus is on helping couples understand and modify their automatic responses to each other, creating a more secure and satisfying relationship.
Historical Context: PACT was developed in the 2000s, drawing on advances in neuroscience and attachment research.
Criticisms:
- Some argue that the approach may be too complex or technical for some couples.
- Critics question whether the neuroscience-based interventions offer significant advantages over traditional couple therapy techniques.
Radically Open Dialectical Behavior Therapy (RO-DBT)
Founder: Thomas R. Lynch
Techniques:
- Social signaling interventions
- Flexible-mind training
- Emotional expression skills
- Open receptivity practices
Focus: The focus is on enhancing social connectedness by targeting maladaptive overcontrol.
Historical Context: RO-DBT was developed in the 2000s as an adaptation of standard DBT to address the needs of individuals with overcontrolled personalities.
Criticisms:
- Some question whether a separate treatment is necessary for overcontrol, as opposed to adapting existing therapies.
- There is ongoing research to establish its effectiveness compared to other treatments for the target disorders.
Rapid Resolution Therapy (RRT)
Founder: Jon Connelly
Techniques:
- Hypnotic induction
- Metaphorical storytelling
- Multi-level communication
- Reimprinting
Focus: The focus is on eliminating the negative emotional or behavioral effects of traumatic events without requiring the client to relive the trauma.
Historical Context: RRT was developed in the early 2000s as a faster alternative to traditional trauma therapies.
Criticisms:
- Some question the rapidity of change claimed by RRT practitioners.
- Critics argue that the approach may not adequately address complex or developmental trauma.
Relational Cultural Therapy (RCT)
Founders: Jean Baker Miller, Judith V. Jordan, Janet Surrey, and Irene Stiver
Techniques:
- Exploration of relational images
- Analysis of power dynamics in relationships
- Fostering mutual empathy and growth-fostering relationships
- Addressing sociocultural contexts of distress
Focus: The focus is on helping clients develop more connected and empowering relationships, recognizing the impact of cultural and societal factors on relational patterns.
Historical Context: RCT was developed in the 1970s and 1980s at the Stone Center at Wellesley College, building on feminist theory and a relational understanding of psychology.
Criticisms:
- Some argue that the approach may overemphasize relational factors at the expense of individual intrapsychic processes.
- Critics question whether the feminist orientation of the therapy limits its applicability to diverse populations.
Resolving Yesterday
Founder: Richard Reeves
Approach: Resolving Yesterday is an approach to healing traumatic memories that combines elements of EMDR, Gestalt therapy, and cognitive techniques.
Techniques:
- Bilateral stimulation
- Empty chair work
- Cognitive restructuring
- Metaphorical representations of trauma resolution
Focus: The focus is on resolving traumatic memories by addressing cognitive, emotional, and somatic aspects of the trauma simultaneously.
Historical Context: Resolving Yesterday was developed in the 1990s, integrating various established therapeutic techniques into a new trauma resolution approach.
Criticisms:
- Some question whether the integration of multiple techniques offers significant advantages over established trauma therapies.
- There is limited empirical research on its effectiveness compared to other trauma-focused approaches.
Reteaming
Founders: Ben Furman and Tapani Ahola
Approach: Reteaming is a solution-focused, goal-oriented approach that helps individuals and groups achieve their goals through a structured, step-by-step process.
Techniques:
- Collaborative goal setting
- Identifying helpers and supporters
- Anticipating and overcoming obstacles
- Celebrating small successes
Focus: The focus is on mobilizing personal and social resources to achieve desired changes, emphasizing teamwork and positive reinforcement.
Historical Context: Reteaming was developed in the 1990s in Finland, building on solution-focused brief therapy principles.
Criticisms:
- Some argue that the approach may oversimplify complex problems by focusing primarily on goals and solutions.
- Critics question whether the structured nature of the process is suitable for all types of issues or clients.
Self-System Therapy (SST)
Founders: Timothy J. Strauman and Kari M. Eddington
Techniques:
- Self-discrepancy assessment
- Goal analysis and revision
- Promotion vs. prevention focus exploration
- Self-regulation skills training
Focus: The focus is on helping clients identify and modify maladaptive self-regulatory patterns, particularly those related to goal pursuit and attainment.
Historical Context: SST was developed in the early 2000s, integrating concepts from self-discrepancy theory and regulatory focus theory with cognitive-behavioral techniques.
Criticisms:
- Some question whether the focus on self-regulation is sufficient to address all aspects of depression.
- There is ongoing research to establish its effectiveness compared to other treatments for depression.
Sensorimotor Art Therapy
Founder: Cornelia Elbrecht
Techniques:
- Body-focused art making
- Tracking sensations during creative process
- Bilateral drawing
- Somatic resourcing through art
Focus: The focus is on using art-making processes to access and integrate sensory and motor experiences, particularly in the treatment of trauma.
Historical Context: Sensorimotor Art Therapy was developed in the 2000s, building on Pat Ogden’s sensorimotor psychotherapy and integrating it with art therapy practices.
Criticisms:
- Some argue that the combination of sensorimotor and art therapy approaches may be too complex for some clients.
- There is limited empirical research on its effectiveness compared to other trauma-focused or art therapy approaches.
Souldrama
Founder: Connie Miller
Techniques:
- Psychodramatic enactment
- Chakra-based interventions
- Spiritual and existential exploration
- Group rituals and ceremonies
Focus: The focus is on helping individuals connect with their higher purpose, resolve internal conflicts, and achieve personal transformation.
Historical Context: Souldrama was developed in the 1990s, combining elements of psychodrama with spiritual and energy-based concepts.
Criticisms:
- Some question the scientific basis for the integration of chakra systems and spiritual principles into psychotherapy.
- Critics argue that the approach may not be suitable for clients who are uncomfortable with spiritual or energy-based concepts.
Systemic Constellations (Family Constellations)
Founder: Bert Hellinger
Techniques:
- Spatial arrangement of representatives
- Observing and interpreting system dynamics
- Releasing sentences
- Rituals of acknowledgment and resolution
Focus: The focus is on identifying and resolving entanglements in family systems that may be influencing current problems.
Historical Context: Systemic Constellations was developed in the 1990s, drawing on elements of family systems therapy, existential phenomenology, and Zulu beliefs.
Criticisms:
- Many critics argue that the approach lacks scientific credibility and empirical support.
- Some question the ethical implications of making claims about family members who are not present.
Time Perspective Therapy (TPT)
Founders: Philip Zimbardo, Richard Sword, and Rosemary Sword
Approach: TPT focuses on understanding and modifying an individual’s time perspective to improve mental health and decision-making.
Techniques:
- Time perspective inventory assessment
- Balancing time perspectives
- Future-oriented goal setting
- Reframing past negative experiences
Focus: The focus is on helping clients develop a more balanced time perspective, reducing the impact of past negative experiences and cultivating a more positive future orientation.
Historical Context: TPT was developed in the 2000s, based on Philip Zimbardo’s research on time perspective and its impact on behavior and mental health.
Criticisms:
- Some argue that the approach may oversimplify complex psychological issues by focusing primarily on time perspective.
- There is limited empirical research on its effectiveness compared to established therapies.
Trauma-Informed Stabilization Treatment (TIST)
Founder: Janina Fisher
Approach: TIST is an approach to treating complex trauma that focuses on stabilization and integration of traumatic memories through body-oriented interventions.
Techniques:
- Sensorimotor interventions
- Parts work
- Mindfulness-based techniques
- Psychoeducation about trauma responses
Focus: The focus is on helping clients develop internal resources and stability before processing traumatic memories.
Historical Context: TIST was developed in the 2000s, integrating concepts from sensorimotor psychotherapy, internal family systems, and cognitive-behavioral approaches.
Criticisms:
- Some argue that the focus on stabilization may delay trauma processing unnecessarily for some clients.
- Critics question whether the integrative nature of the approach makes it difficult to isolate effective components.
Unified Protocol for Transdiagnostic Treatment of Emotional Disorders (UP)
Founders: David H. Barlow and colleagues
Approach: UP is a cognitive-behavioral treatment that applies core therapeutic principles to a wide range of emotional disorders.
Techniques:
- Mindful emotion awareness
- Cognitive flexibility
- Emotion exposure
- Countering emotional behaviors
Focus: The focus is on addressing common underlying processes across emotional disorders rather than disorder-specific symptoms.
Historical Context: UP was developed in the 2000s as a response to high comorbidity rates among emotional disorders and the need for more efficient treatment approaches.
Criticisms:
- Some question whether a transdiagnostic approach can be as effective as disorder-specific treatments.
- Critics argue that the approach may not adequately address unique features of specific disorders.
Video-feedback Intervention to promote Positive Parenting (VIPP)
Founders: Femmie Juffer, Marian J. Bakermans-Kranenburg, and Marinus H. van IJzendoorn
Approach: VIPP is a short-term, attachment-based intervention that uses video feedback to enhance parental sensitivity and positive parent-child interactions.
Techniques:
- Video recording of parent-child interactions
- Guided review and discussion of interactions
- Reinforcement of positive parenting behaviors
- Psychoeducation on child development and attachment
Focus: The focus is on improving parental sensitivity and responsiveness to promote secure attachment in young children.
Historical Context: VIPP was developed in the 1990s at Leiden University, based on attachment theory and research on early parent-child interactions.
Criticisms:
- Some argue that the short-term nature of the intervention may not be sufficient for families with complex issues.
- Critics question whether improvements in observed interactions necessarily translate to long-term changes in attachment security.
Waking Dream Therapy
Key Figure: Gerald Epstein
Approach: Waking Dream Therapy uses guided imagery in a waking state to access and work with unconscious material, similar to dream analysis.
Techniques:
- Guided waking dream experiences
- Symbolic interpretation
- Active imagination
- Integration of insights into daily life
Focus: The focus is on accessing the wisdom of the unconscious mind to gain insights and promote healing.
Historical Context: Waking Dream Therapy was developed in the mid-20th century, influenced by Jung’s active imagination technique and European traditions of guided imagery.
Criticisms:
- Some argue that the approach may be too abstract or esoteric for clients seeking more concrete interventions.
- Critics question the validity of symbolic interpretations made in waking dream experiences.
Wilderness Therapy
Key Figures: Kurt Hahn, Larry Dean Olsen
Approach: Wilderness Therapy uses outdoor experiences and nature-based challenges to promote personal growth, self-reliance, and therapeutic change.
Techniques:
- Outdoor survival skills training
- Group process activities
- Solo experiences in nature
- Metaphorical learning from natural environments
Focus: The focus is on using the challenges and experiences of wilderness settings to foster personal development, improve self-esteem, and address behavioral issues.
Historical Context: While therapeutic use of wilderness experiences has ancient roots, modern Wilderness Therapy programs began to develop in the 1960s and gained popularity in the 1990s.
Criticisms:
- Some question the safety and ethical considerations of removing clients from their usual environments.
- Critics argue that gains made in wilderness settings may not generalize to everyday life.
Writing Therapy
Key Figures: James Pennebaker, Ira Progoff
Approach: Writing Therapy uses various forms of written expression as a means of therapeutic exploration and healing.
Techniques:
- Expressive writing about traumatic experiences
- Structured journaling exercises
- Poetry therapy
- Letter writing (unsent letters)
Focus: The focus is on using writing to process emotions, gain insights, and promote healing from various psychological issues.
Historical Context: While writing has been used therapeutically throughout history, modern Writing Therapy techniques gained prominence in the latter half of the 20th century.
Criticisms:
- Some argue that writing therapy may not be suitable for individuals with limited literacy or those who find writing stressful.
- Critics question whether insights gained through writing consistently translate into behavioral change.
Yoga Therapy
Key Figures: Swami Kuvalyananda, T.K.V. Desikachar
Techniques:
- Asana (physical postures)
- Pranayama (breathing exercises)
- Meditation and mindfulness practices
- Application of yogic philosophy to daily life
Focus: The focus is on integrating body, mind, and spirit to address various physical and mental health issues and promote overall well-being.
Historical Context: While yoga has ancient roots, its application as a formal therapy gained recognition in the 20th century and has grown significantly in recent decades.
Criticisms:
- Some question whether the spiritual aspects of yoga are appropriate in a therapeutic context.
- Critics argue that the physical practices may not be suitable for all clients, particularly those with certain health conditions.
Zero Balancing
Founder: Fritz Smith
Techniques:
- Gentle finger pressure and stretching
- Working with “fulcrums” or points of balanced tension
- Attention to bone energy
- Integration of body-mind experiences
Focus: The focus is on promoting physical and emotional balance by working with the body’s energy fields and structural system.
Historical Context: Zero Balancing was developed in the 1970s, integrating Western scientific approaches with Eastern energy concepts.
Criticisms:
- Some question the scientific basis for the energy concepts used in Zero Balancing.
- Critics argue that the effects may be due to general touch and relaxation rather than specific energy work.
Psychodynamic Therapy
Key Figures: Sigmund Freud, Carl Jung, Melanie Klein, Otto Kernberg
Techniques:
Free association Dream analysis Transference interpretation Exploration of defense mechanisms
Focus: The focus is on gaining insight into unconscious conflicts, patterns, and motivations that contribute to emotional distress and interpersonal difficulties.
Historical Context: Psychodynamic therapy originated with Sigmund Freud’s psychoanalysis in the late 19th and early 20th centuries and has since evolved into various schools and approaches.
Criticisms:
Some argue that psychodynamic therapy may be too time-consuming or expensive for many clients. Critics question the scientific validity and empirical support for some psychodynamic concepts and techniques.
Humanistic Therapy
Key Figures: Carl Rogers, Abraham Maslow, Rollo May
Approach: Humanistic therapy emphasizes the importance of self-actualization, personal growth, and the inherent human capacity for healing and fulfillment.
Techniques:
Active listening and empathy Unconditional positive regard Facilitating self-exploration and awareness Focus on the here-and-now experience
Focus: The focus is on helping clients develop self-awareness, self-acceptance, and the ability to live authentically and in accordance with their own values and aspirations.
Historical Context: Humanistic therapy emerged in the 1950s and 1960s as a “third force” in psychology, alongside psychoanalysis and behaviorism, with key figures including Carl Rogers and Abraham Maslow.
Criticisms:
Some argue that humanistic therapy may lack clear structure or specific techniques for addressing certain mental health conditions. Critics question the empirical support for some humanistic concepts and the effectiveness of these therapies compared to other established approaches.
Integrative Therapy
Key Figures: Arnold Lazarus, Paul Wachtel, John Norcross
Approach: Integrative therapy combines elements from different theoretical orientations and techniques to create a holistic and personalized treatment approach tailored to the client’s needs and preferences.
Techniques:
Varies depending on the specific integration Common elements may include: Establishing a strong therapeutic relationship Collaborative goal-setting and treatment planning Flexibility in the use of techniques and interventions Attention to client feedback and progress
Focus: The focus is on providing a comprehensive and individualized treatment approach that draws on the strengths of multiple therapeutic perspectives.
Historical Context: Integrative approaches gained prominence in the 1970s and 1980s as a response to the limitations of single-school approaches and the recognition of common factors across therapies.
Criticisms:
Some argue that integrative approaches may lack a coherent theoretical foundation or may be difficult to operationalize and research. Critics question the training and competence of therapists in multiple theoretical orientations and techniques.
Interpersonal Therapy (IPT)
Founders: Gerald Klerman, Myrna Weissman
Approach: IPT is a time-limited therapy that focuses on improving interpersonal functioning to alleviate symptoms of depression and other mental health conditions.
Techniques:
Identification of interpersonal problem areas (grief, role disputes, role transitions, interpersonal deficits) Communication analysis and skills training Exploration of relationship patterns and expectations Encouraging the development of social support
Focus: The focus is on helping clients understand and modify problematic interpersonal patterns that contribute to their distress, and to develop more satisfying and supportive relationships.
Historical Context: IPT was developed in the 1970s as a treatment for depression, based on the idea that depression often occurs in an interpersonal context.
Criticisms:
Some argue that IPT may not adequately address other factors contributing to mental health issues, such as cognitive or biological factors. Critics question the long-term effectiveness of IPT and its applicability to a wide range of mental health conditions.
Family Systems Therapy
Key Figures: Murray Bowen, Virginia Satir, Salvador Minuchin, Jay Haley
Approach: Family systems therapy views individual problems as manifestations of dysfunctional family dynamics and seeks to promote change by altering these patterns of interaction.
Techniques:
Family mapping or genograms Reframing and relabeling Structural interventions (e.g., boundaries, subsystems) Circular questioning and feedback
Focus: The focus is on improving communication, resolving conflicts, and fostering healthier patterns of relating within the family system.
Historical Context: Family systems therapy emerged in the 1950s and 1960s, with key approaches including Bowen family systems theory, structural family therapy, and strategic family therapy.
Criticisms:
Some argue that family systems therapy may not adequately address individual psychological factors or issues outside the family context. Critics question the applicability of family systems concepts to diverse family structures and cultural backgrounds.
Solution-Focused Brief Therapy (SFBT)
Founders: Steve de Shazer, Insoo Kim Berg
Approach: SFBT is a short-term, goal-oriented therapy that focuses on identifying and amplifying clients’ strengths, resources, and exceptions to their problems to facilitate positive change.
Techniques:
Miracle question and scaling questions Exception-finding and coping questions Compliments and positive feedback Homework assignments and experiments
Focus: The focus is on helping clients envision and work towards their desired future outcomes, rather than dwelling on past problems or pathology.
Historical Context: SFBT was developed in the late 1970s and 1980s at the Brief Family Therapy Center in Milwaukee, Wisconsin, by Steve de Shazer, Insoo Kim Berg, and their colleagues.
Criticisms:
Some argue that SFBT may not adequately address severe or complex mental health issues that require more in-depth exploration. Critics question the long-term effectiveness of SFBT and its applicability to clients who have difficulty envisioning or articulating their goals.
Narrative Therapy
Founders: Michael White, David Epston
Approach: Narrative therapy views problems as separate from people and helps clients “re-author” their life stories to create more empowering and satisfying narratives.
Techniques:
Externalization of the problem Deconstruction of dominant narratives Unique outcomes and alternative stories Therapeutic documents and certificates Outsider-witness practices and re-membering conversations
Focus: The focus is on helping clients challenge and reframe oppressive or limiting narratives, and to develop a stronger sense of agency, identity, and connection to their preferred values and relationships.
Historical Context: Narrative therapy was developed in the 1980s and 1990s by Michael White and David Epston, influenced by postmodern and social constructionist philosophy.
Criticisms:
Some argue that narrative therapy may not adequately address biological or psychological factors contributing to mental health issues. Critics question the effectiveness of narrative therapy for clients who have difficulty with abstract or metaphorical thinking.
Problem-Solving Therapy (PST)
Founders: Thomas D’Zurilla, Arthur Nezu
Approach: PST is a brief, structured intervention that teaches individuals a systematic approach to identifying and solving problems in their lives, with the goal of reducing psychological distress and enhancing coping skills.
Techniques:
Problem orientation and definition Generation of alternative solutions Decision-making and solution implementation Outcome evaluation and verification Relapse prevention and generalization
Focus: The focus is on helping clients develop a more positive and effective problem-solving orientation, as well as specific problem-solving skills that they can apply to a wide range of life challenges.
Historical Context: PST was developed in the 1970s and 1980s by Thomas D’Zurilla and Arthur Nezu, drawing on cognitive-behavioral principles and the idea that deficits in problem-solving can contribute to psychological distress.
Criticisms:
Some argue that PST may be too simplistic or mechanistic for complex, chronic, or emotionally-charged problems. Critics question the long-term durability of treatment gains and the applicability of PST to severe mental health conditions.
Mindfulness-Based Cognitive Therapy (MBCT)
Founders: Zindel Segal, Mark Williams, John Teasdale
Approach: MBCT is an evidence-based group intervention that combines elements of cognitive-behavioral therapy with mindfulness practices to prevent relapse in individuals with a history of depression.
Techniques:
Formal and informal mindfulness practices Body scans and yoga Exploration of automatic thought patterns Development of a decentered perspective on thoughts Relapse prevention planning
Focus: The focus is on helping clients develop a more accepting and non-reactive relationship with their thoughts and feelings, particularly those associated with depressive relapse, and to engage in self-care and positive coping strategies.
Historical Context: MBCT was developed in the 1990s by Zindel Segal, Mark Williams, and John Teasdale, adapting Jon Kabat-Zinn’s mindfulness-based stress reduction (MBSR) program for use with formerly depressed individuals.
Criticisms:
Some argue that MBCT may not be suitable for individuals in the midst of an acute depressive episode or those with severe symptoms. Critics question the incremental effectiveness of MBCT beyond standard cognitive-behavioral interventions for depression.
Metacognitive Therapy (MCT)
Founder: Adrian Wells
Approach: MCT is a cognitive-behavioral approach that focuses on modifying maladaptive metacognitive beliefs and processes (i.e., thoughts about thinking) that maintain psychological distress.
Techniques:
Socialization to the metacognitive model Detached mindfulness and attention training Challenging positive and negative metacognitive beliefs Behavioral experiments and worry/rumination postponement Relapse prevention and generalization
Focus: The focus is on helping clients develop a more flexible and detached relationship with their thoughts, reduce perseverative thinking patterns (such as worry and rumination), and strengthen metacognitive control and resilience.
Historical Context: MCT was developed in the 1990s and 2000s by Adrian Wells and his colleagues, drawing on advances in cognitive psychology and the role of metacognition in emotional disorders.
Criticisms:
Some argue that MCT’s emphasis on metacognition may not adequately address other important factors contributing to psychological distress. Critics question the unique contributions of MCT beyond standard cognitive-behavioral interventions.
Rational Emotive Behavior Therapy (REBT)
Founder: Albert Ellis
Techniques:
Disputation of irrational beliefs Cognitive restructuring and reframing Behavioral experiments and exposure Unconditional self-acceptance and frustration tolerance Rational emotive imagery and role-playing
Focus: The focus is on helping clients develop more rational and adaptive ways of thinking, emote more appropriately, and behave more effectively in the face of life challenges.
Historical Context: REBT was developed in the 1950s and 1960s by Albert Ellis, and is considered one of the first cognitive-behavioral therapies.
Criticisms:
Some argue that REBT’s emphasis on rationality and disputation may not adequately address emotional or experiential factors. Critics question the philosophical assumptions underlying REBT and the empirical support for some of its specific techniques.
Gottman Method Couples Therapy
Founders: John Gottman, Julie Schwartz Gottman
Techniques:
Assessment of relationship strengths and challenges Interventions to enhance friendship and intimacy Emotion coaching and stress management Addressing negative conflict patterns (e.g., criticism, defensiveness) Facilitating meaningful shared experiences
Focus: The focus is on helping couples build a strong foundation of friendship, navigate conflicts constructively, and cultivate a sense of shared purpose and meaning in their lives together.
Historical Context: The Gottman Method was developed in the 1990s and 2000s by John Gottman and Julie Schwartz Gottman, based on extensive research on the predictors of relationship success and stability.
Criticisms:
Some argue that the Gottman Method may not adequately address deep-seated individual or intergenerational issues affecting the relationship. Critics question the applicability of the Gottman Method to diverse couple populations and the long-term effectiveness of the interventions.
Imago Relationship Therapy
Founder: Harville Hendrix
Approach: Imago Relationship Therapy is a couples therapy approach that focuses on understanding and healing childhood wounds that affect adult relationships, with the goal of fostering personal growth and relationship satisfaction.
Techniques:
Dialogue process for safe communication Exploration of childhood experiences and unmet needs Re-imagining and restructuring frustrations Behavioral changes and positive interactions Developing shared relationship vision
Focus: The focus is on helping couples understand how their early experiences and unconscious “imago” (image of familiar love) shape their choice of partner and relationship dynamics, and to consciously co-create a more fulfilling and growth-fostering relationship.
Historical Context: Imago Relationship Therapy was developed in the 1980s by Harville Hendrix and his wife, Helen LaKelly Hunt, integrating insights from psychodynamic, behavioral, and humanistic approaches.
Criticisms:
Some argue that Imago Relationship Therapy’s emphasis on childhood experiences may not adequately address present-day relationship challenges. Critics question the empirical support for some of the key concepts and techniques used in Imago Relationship Therapy.
Integrative Behavioral Couple Therapy (IBCT)
Founders: Neil S. Jacobson, Andrew Christensen
Techniques:
Behavioral exchange and problem-solving Acceptance and tolerance of relationship differences Empathic joining and unified detachment Identification of core conflictual relationship themes Dyadic coping and stress management
Focus: The focus is on helping couples increase positive interactions, develop greater acceptance and understanding of each other’s differences, and work together to manage stressors and conflicts.
Historical Context: IBCT was developed in the 1990s by Neil S. Jacobson and Andrew Christensen, integrating traditional behavioral couple therapy with insights from acceptance-based approaches.
Criticisms:
Some argue that IBCT’s emphasis on acceptance may not adequately address severe or entrenched relationship problems. Critics question the long-term durability of treatment gains and the applicability of IBCT to diverse couple populations.
Emotion-Focused Therapy for Couples (EFT-C)
Founders: Leslie Greenberg, Susan Johnson
Approach: EFT-C is an evidence-based approach to couples therapy that focuses on identifying and changing negative interactional patterns and fostering secure attachment bonds between partners.
Techniques:
Identifying and deescalating negative cycles Accessing and reprocessing primary emotions Restructuring interactions and promoting emotional engagement Fostering expression of attachment needs and responsiveness Consolidating new interactional patterns
Focus: The focus is on helping couples create a more secure and satisfying relationship by transforming negative cycles of interaction into positive cycles of accessibility, responsiveness, and engagement.
Historical Context: EFT-C was developed in the 1980s and 1990s by Leslie Greenberg and Susan Johnson, integrating humanistic, systemic, and attachment theories.
Criticisms:
Some argue that EFT-C may not adequately address individual psychological factors or issues outside the couple’s relationship. Critics question the applicability of EFT-C to diverse couple populations and the long-term stability of treatment gains.
Motivational Interviewing (MI)
Founders: William R. Miller, Stephen Rollnick
Approach: MI is a client-centered, directive approach that helps individuals explore and resolve ambivalence about behavior change and strengthen their intrinsic motivation to change.
Techniques:
Open-ended questions Affirmations Reflective listening Summaries Eliciting change talk
Focus: The focus is on creating a collaborative, non-judgmental atmosphere that allows clients to explore their own reasons for change and develop a sense of autonomy and self-efficacy.
Historical Context: MI was developed in the 1980s by William R. Miller, initially as a brief intervention for problem drinking. It has since been adapted for a wide range of health behaviors and settings.
Criticisms:
Some argue that MI may not be sufficient as a standalone treatment for more severe or complex substance use disorders. Critics question the effectiveness of MI for clients who have low intrinsic motivation or limited verbal communication skills.
Acceptance and Commitment Therapy (ACT)
Founders: Steven C. Hayes, Kelly G. Wilson, Kirk Strosahl
Approach: ACT is a contextual cognitive-behavioral approach that emphasizes mindfulness, acceptance, and values-based action to promote psychological flexibility and well-being.
Techniques:
Acceptance and willingness exercises Cognitive defusion techniques Values clarification and committed action Mindfulness practices Experiential metaphors and paradoxes
Focus: The focus is on helping clients develop a more accepting and mindful relationship with their thoughts and feelings, while clarifying and pursuing their values and goals.
Historical Context: ACT was developed in the 1980s and 1990s by Steven C. Hayes and his colleagues, drawing on behavioral analysis, cognitive therapy, and Eastern philosophical traditions.
Criticisms:
Some argue that ACT’s philosophical underpinnings may be too abstract or esoteric for certain clients. Critics question the unique contributions of ACT beyond traditional cognitive-behavioral therapy.
Schema Therapy
Founders: Jeffrey Young, Janet Klosko, Marjorie Weishaar
Approach: Schema therapy is an integrative approach that combines elements of cognitive, behavioral, and psychodynamic therapies to address deep-rooted patterns of thinking, feeling, and behaving that originate in childhood and contribute to psychological distress.
Techniques:
Identifying and challenging maladaptive schemas Experiential techniques (e.g., imagery rescripting, chair dialogues) Limited reparenting Behavioral pattern-breaking Cognitive restructuring
Focus: The focus is on helping clients identify and modify self-defeating life patterns, develop healthier coping mechanisms, and meet their core emotional needs in adaptive ways.
Historical Context: Schema therapy was developed in the 1980s and 1990s by Jeffrey Young, initially as a treatment for personality disorders and chronic characterological issues.
Criticisms:
Some argue that schema therapy’s integration of multiple theoretical orientations may lack parsimony or coherence. Critics question the empirical support for specific schema therapy techniques and the long-term effectiveness of the approach.
Cognitive Processing Therapy (CPT)
Founders: Patricia Resick, Candice Monson, Kathleen Chard
Approach: CPT is a structured, evidence-based treatment for posttraumatic stress disorder (PTSD) that focuses on identifying and modifying maladaptive beliefs related to traumatic experiences.
Techniques:
Psychoeducation about PTSD and cognitive theory Identification and challenging of stuck points Trauma narrative writing and processing Cognitive restructuring Safety, trust, power/control, esteem, intimacy beliefs
Focus: The focus is on helping clients process and make sense of their traumatic experiences, while developing more balanced and adaptive beliefs about themselves, others, and the world.
Historical Context: CPT was developed in the 1980s and 1990s by Patricia Resick and her colleagues, adapting cognitive therapy principles to the treatment of PTSD.
Criticisms:
Some argue that CPT’s focus on cognitive factors may not adequately address the emotional and physiological aspects of trauma. Critics question the appropriateness of CPT for complex or prolonged trauma and its effectiveness compared to other evidence-based PTSD treatments.
Eye Movement Desensitization and Reprocessing (EMDR)
Founder: Francine Shapiro
Techniques:
History-taking and treatment planning Preparation and stabilization Assessment and desensitization of target memories Installation of positive cognition Body scan and closure Re-evaluation
Focus: The focus is on helping clients reprocess traumatic experiences, reduce distress, and develop more adaptive beliefs and coping mechanisms.
Historical Context: EMDR was developed in the late 1980s by Francine Shapiro, based on her observation that eye movements seemed to reduce the intensity of disturbing thoughts.
Criticisms:
Some argue that the theoretical mechanisms underlying EMDR (e.g., bilateral stimulation) are not well-established or empirically supported. Critics question whether eye movements or other forms of bilateral stimulation are necessary components of the therapy, as opposed to other common factors.
Prolonged Exposure Therapy (PE)
Founder: Edna B. Foa
Approach: PE is an evidence-based treatment for PTSD that involves gradual, repeated exposure to trauma-related memories, situations, and sensations to reduce fear and avoidance and promote emotional processing.
Techniques:
Psychoeducation about PTSD and rationale for exposure In vivo exposure to avoided situations Imaginal exposure to traumatic memories Processing of thoughts and feelings related to exposure Breathing retraining
Focus: The focus is on helping clients confront and habituate to trauma-related stimuli, thereby reducing symptoms of PTSD and improving overall functioning.
Historical Context: PE was developed in the 1980s and 1990s by Edna B. Foa and her colleagues, drawing on the principles of emotional processing theory and habituation.
Criticisms:
Some argue that PE may be too intense or distressing for certain clients, particularly those with severe or complex trauma histories. Critics question the long-term durability of treatment gains and the potential for symptom exacerbation during the course of PE.
Cognitive Behavioral Analysis System of Psychotherapy (CBASP)
Founder: James P. McCullough Jr.
Approach: CBASP is a time-limited, integrative treatment approach specifically designed for chronic depression that combines elements of cognitive, behavioral, and interpersonal therapies.
Techniques:
Situational analysis Interpersonal discrimination exercise Behavioral skill training and rehearsal Contingent personal responsivity Disciplined personal involvement
Focus: The focus is on helping clients with chronic depression understand the consequences of their behavior, develop more effective interpersonal skills, and increase their sense of self-efficacy and interpersonal empowerment.
Historical Context: CBASP was developed in the 1990s by James P. McCullough Jr., based on his observation that traditional CBT approaches were less effective for chronic depression.
Criticisms:
Some argue that CBASP’s integration of multiple theoretical orientations may be too complex or unwieldy for certain clients or settings. Critics question the unique contributions of CBASP beyond other established treatments for chronic depression.
Internal Family Systems (IFS)
Founder: Richard C. Schwartz
Techniques:
Identifying and differentiating parts Developing a relationship with parts Accessing and strengthening the Self Unburdening and healing wounded parts Facilitating internal dialogue and negotiation
Focus: The focus is on helping clients develop greater self-awareness, self-compassion, and inner peace by understanding and integrating the different aspects of their psyche.
Historical Context: IFS was developed in the 1980s and 1990s by Richard C. Schwartz, drawing on his experience with family therapy and systems thinking.
Criticisms:
Some argue that IFS’s conceptualization of the mind as consisting of distinct parts may not be empirically supported or may oversimplify the complexity of human experience. Critics question the long-term effectiveness of IFS and its applicability to severe or acute mental health conditions.
Functional Analytic Psychotherapy (FAP)
Founders: Robert J. Kohlenberg, Mavis Tsai
Techniques:
Identifying clinically relevant behaviors (CRBs) Evoking and reinforcing positive CRBs Observing and responding to in-session interpersonal dynamics Generalization of in-session gains to daily life Functional analysis of out-of-session behavior
Focus: The focus is on helping clients develop more effective interpersonal skills and ways of relating by using the therapeutic relationship as a microcosm for real-world interactions.
Historical Context: FAP was developed in the 1980s and 1990s by Robert J. Kohlenberg and Mavis Tsai, drawing on principles of behavior analysis and the importance of the therapeutic alliance.
Criticisms:
Some argue that FAP’s emphasis on the therapeutic relationship may blur professional boundaries or create dependency. Critics question the generalizability of in-session behavior change to clients’ daily lives and the long-term effectiveness of the approach.
Integrative Behavioral Couple Therapy (IBCT)
Founders: Neil S. Jacobson, Andrew Christensen
Techniques:
Behavioral exchange and problem-solving Acceptance and tolerance of relationship differences Empathic joining and unified detachment Identification of core conflictual relationship themes Dyadic coping and stress management
Focus: The focus is on helping couples increase positive interactions, develop greater acceptance and understanding of each other’s differences, and work together to manage stressors and conflicts.
Historical Context: IBCT was developed in the 1990s by Neil S. Jacobson and Andrew Christensen, integrating traditional behavioral couple therapy with insights from acceptance-based approaches.
Criticisms:
Some argue that IBCT’s emphasis on acceptance may not adequately address severe or entrenched relationship problems. Critics question the long-term durability of treatment gains and the applicability of IBCT to diverse couple populations.
Behavioral Activation (BA)
Founders: Neil S. Jacobson, Peter M. Lewinsohn
Approach: BA is a structured, evidence-based treatment for depression that focuses on increasing engagement in rewarding activities and reducing avoidance behaviors.
Techniques:
Activity monitoring and scheduling Graded task assignment Problem-solving obstacles to activation Contingency management Values assessment and goal-setting
Focus: The focus is on helping clients re-engage with positive reinforcers in their environment, develop a sense of mastery and accomplishment, and improve their overall mood and functioning.
Historical Context: BA has its roots in the behavioral models of depression developed by Peter M. Lewinsohn and others in the 1970s. It was formalized as a standalone treatment by Neil S. Jacobson and colleagues in the 1990s.
Criticisms:
Some argue that BA may not adequately address cognitive or interpersonal factors contributing to depression. Critics question the long-term effectiveness of BA and its applicability to severe or recurrent forms of depression.
Cognitive Behavioral Therapy (CBT)
Founders: Aaron Beck, Albert Ellis
Approach: CBT is a structured, short-term therapy that focuses on identifying and modifying maladaptive thoughts and behaviors to improve emotional well-being.
Techniques:
Cognitive restructuring Behavioral activation Exposure therapy Skills training (e.g., relaxation, assertiveness)
Focus: The focus is on helping clients develop more adaptive and flexible ways of thinking and behaving to reduce distress and improve functioning.
Historical Context: CBT emerged in the 1960s and 1970s, with Aaron Beck’s cognitive therapy and Albert Ellis’s rational emotive behavior therapy (REBT) being the two main branches.
Criticisms:
Some argue that CBT may not adequately address deeper emotional or unconscious processes. Critics question the long-term effectiveness of CBT and its applicability to more complex or severe mental health conditions.
Psychodynamic Therapy
Key Figures: Sigmund Freud, Carl Jung, Melanie Klein
Approach: Psychodynamic therapy is a broad term for therapies that focus on unconscious processes, early childhood experiences, and the dynamics of the therapist-client relationship.
Techniques:
Free association Dream analysis Transference interpretation Exploration of defense mechanisms
Focus: The focus is on gaining insight into unconscious conflicts, patterns, and motivations that contribute to emotional distress and interpersonal difficulties.
Historical Context: Psychodynamic therapy originated with Sigmund Freud’s psychoanalysis in the late 19th and early 20th centuries and has since evolved into various schools and approaches.
Criticisms:
Some argue that psychodynamic therapy may be too time-consuming or expensive for many clients. Critics question the scientific validity and empirical support for some psychodynamic concepts and techniques.
Humanistic-Experiential Therapies
Key Figures: Carl Rogers, Fritz Perls, Irving Yalom
Approach: Humanistic-experiential therapies emphasize the importance of self-actualization, personal growth, and the authentic expression of emotions in the therapeutic process.
Techniques:
Active listening and reflection Experiential exercises and role-plays Focusing on the here-and-now Exploration of existential concerns
Focus: The focus is on helping clients develop self-awareness, authenticity, and a sense of meaning and purpose in life.
Historical Context: Humanistic-experiential therapies emerged in the 1950s and 1960s as part of the “third force” in psychology, with key approaches including person-centered therapy, Gestalt therapy, and existential therapy.
Criticisms:
Some argue that humanistic-experiential therapies may lack clear structure or specific techniques for addressing certain mental health conditions. Critics question the empirical support for some humanistic-experiential concepts and the effectiveness of these therapies compared to other established approaches.
Family Systems Therapy
Key Figures: Murray Bowen, Virginia Satir, Salvador Minuchin
Approach: Family systems therapy views individual problems as manifestations of dysfunctional family dynamics and seeks to promote change by altering these patterns of interaction.
Techniques:
Family mapping or genograms Reframing and relabeling Structural interventions (e.g., boundaries, subsystems) Experiential exercises and role-plays
Focus: The focus is on improving communication, resolving conflicts, and fostering healthier patterns of relating within the family system.
Historical Context: Family systems therapy emerged in the 1950s and 1960s, with key approaches including Bowen family systems theory, structural family therapy, and strategic family therapy.
Criticisms:
Some argue that family systems therapy may not adequately address individual psychological factors or issues outside the family context. Critics question the applicability of family systems concepts to diverse family structures and cultural backgrounds.
Group Therapy
Key Figures: Irvin Yalom, J. L. Moreno
Approach: Group therapy involves the use of group dynamics and interactions to promote personal growth, interpersonal learning, and therapeutic change.
Techniques:
Group cohesion building Interpersonal feedback and confrontation Role-playing and psychodrama Exploration of common themes and experiences
Focus: The focus is on helping clients develop self-awareness, communication skills, and social support through the experience of being part of a therapeutic group.
Historical Context: Group therapy has roots in the early 20th century, with key influences including J. L. Moreno’s psychodrama and Kurt Lewin’s group dynamics. It gained wider popularity in the 1960s and 1970s.
Criticisms:
Some argue that group therapy may not be suitable for clients with severe or acute mental health issues. Critics question the effectiveness of group therapy compared to individual therapy for certain conditions or populations.
Interpersonal Therapy (IPT)
Founders: Gerald Klerman, Myrna Weissman
Approach: IPT is a time-limited therapy that focuses on improving interpersonal functioning to alleviate symptoms of depression and other mental health conditions.
Techniques:
Identification of interpersonal problem areas Role transitions Grief and loss Interpersonal disputes Interpersonal deficits Communication analysis and skills training
Focus: The focus is on helping clients understand and modify problematic interpersonal patterns that contribute to their distress.
Historical Context: IPT was developed in the 1970s as a treatment for depression, based on the idea that depression often occurs in an interpersonal context.
Criticisms:
Some argue that IPT may not adequately address other factors contributing to mental health issues, such as cognitive or biological factors. Critics question the long-term effectiveness of IPT and its applicability to a wide range of mental health conditions.
Dialectical Behavior Therapy (DBT)
Founder: Marsha Linehan
Techniques:
Mindfulness skills training Distress tolerance skills Emotion regulation skills Interpersonal effectiveness skills Behavioral chain analysis
Focus: The focus is on helping clients develop skills to manage intense emotions, tolerate distress, and build a life worth living.
Historical Context: DBT was developed in the 1980s by Marsha Linehan, initially as a treatment for borderline personality disorder and chronic suicidality.
Criticisms:
Some argue that DBT may be too intensive or demanding for certain clients or treatment settings. Critics question the effectiveness of DBT for conditions other than borderline personality disorder.
Mindfulness-Based Therapies
Key Figures: Jon Kabat-Zinn, Zindel Segal, Mark Williams
Approach: Mindfulness-based therapies incorporate mindfulness practices and principles into the therapeutic process to promote self-awareness, emotion regulation, and well-being.
Techniques:
Formal and informal mindfulness practices Body scans and yoga Exploration of automatic thought patterns Acceptance and non-judgment of present-moment experiences
Focus: The focus is on helping clients develop a more accepting and non-reactive relationship with their thoughts, emotions, and physical sensations.
Historical Context: Mindfulness-based therapies emerged in the 1970s and 1980s, with Jon Kabat-Zinn’s mindfulness-based stress reduction (MBSR) program being a key influence. Other approaches include mindfulness-based cognitive therapy (MBCT) and acceptance and commitment therapy (ACT).
Criticisms:
Some argue that mindfulness-based therapies may not adequately address underlying psychological or interpersonal issues. Critics question the long-term effectiveness of mindfulness-based interventions and their applicability to severe mental health conditions.
Integrative and Eclectic Therapies
Key Figures: Arnold Lazarus, Larry E. Beutler, John C. Norcross
Approach: Integrative and eclectic therapies combine elements from different theoretical orientations and techniques to create a personalized treatment approach tailored to the client’s needs and preferences.
Techniques:
Varies depending on the specific integration or eclecticism Common elements may include: Establishing a strong therapeutic relationship Collaborative goal-setting and treatment planning Flexibility in the use of techniques and interventions Attention to client feedback and progress
Focus: The focus is on providing a comprehensive and individualized treatment approach that draws on the strengths of multiple therapeutic perspectives.
Historical Context: Integrative and eclectic approaches gained prominence in the 1970s and 1980s as a response to the limitations of single-school approaches and the recognition of common factors across therapies.
Criticisms:
Some argue that integrative and eclectic approaches may lack a coherent theoretical foundation or may be difficult to operationalize and research. Critics question the training and competence of therapists in multiple theoretical orientations and techniques.
Solution-Focused Brief Therapy (SFBT)
Founders: Steve de Shazer, Insoo Kim Berg
Techniques:
Miracle question Scaling questions Exception-finding questions Compliments and affirmations Homework assignments
Focus: The focus is on helping clients envision and work towards their desired future outcomes, rather than dwelling on past problems or pathology.
Historical Context: SFBT was developed in the 1970s and 1980s at the Brief Family Therapy Center in Milwaukee, Wisconsin, by Steve de Shazer, Insoo Kim Berg, and their colleagues.
Criticisms:
Some argue that SFBT may not adequately address severe or complex mental health issues that require more in-depth exploration. Critics question the long-term effectiveness of SFBT and its applicability to clients who have difficulty envisioning or articulating their goals.
Narrative Therapy
Founders: Michael White, David Epston
Techniques:
Externalization of the problem Deconstruction of dominant narratives Unique outcomes and alternative stories Therapeutic letter writing Outsider witness practices
Focus: The focus is on helping clients challenge and reframe oppressive or limiting narratives and develop a stronger sense of agency and identity.
Historical Context: Narrative therapy was developed in the 1980s and 1990s by Michael White and David Epston, influenced by postmodern and social constructionist philosophy.
Criticisms:
Some argue that narrative therapy may not adequately address biological or psychological factors contributing to mental health issues. Critics question the effectiveness of narrative therapy for clients who have difficulty with abstract or metaphorical thinking.
Developmental Somatic Psychotherapy
Founder: Ruella Frank
Approach: Developmental Somatic Psychotherapy is a body-oriented approach that emphasizes the role of early movement patterns in shaping psychological development and relational patterns.
Techniques:
Embodied movement analysis Developmental movement patterning Touch and tactile exploration Mindfulness and body awareness
Focus: The focus is on exploring and transforming developmental movement patterns to promote psychological integration, self-regulation, and relational capacities.
Historical Context: Developmental Somatic Psychotherapy was developed by Ruella Frank in the 1980s and 1990s, drawing on somatic psychology, developmental psychology, and dance/movement therapy.
Criticisms:
Some argue that the approach may be too focused on early developmental experiences at the expense of present-day concerns. Critics question the empirical support for the role of movement patterns in shaping psychological development.
Dialectical Behavior Therapy for Substance Use Disorders (DBT-SUD)
Founders: Linda Dimeff, Marsha Linehan
Approach: DBT-SUD is an adaptation of standard DBT that focuses on treating individuals with co-occurring substance use disorders and borderline personality disorder.
Techniques:
Mindfulness and distress tolerance skills Emotion regulation and interpersonal effectiveness skills Dialectical abstinence Behavioral chain analysis of substance use
Focus: The focus is on helping clients develop the skills needed to manage intense emotions, reduce substance use, and build a life worth living.
Historical Context: DBT-SUD was developed in the 1990s and 2000s, in response to the high rates of substance use disorders among individuals with borderline personality disorder.
Criticisms:
Some argue that the approach may be too demanding or complex for clients with severe substance use disorders. Critics question the effectiveness of DBT-SUD compared to other established treatments for substance use disorders.
Dialogical Gestalt Therapy
Founder: Wolfgang Rechberger
Techniques:
Here-and-now focus Experimentation and creative adjustment Dialogue and inclusion Field-theoretical exploration
Focus: The focus is on exploring the client’s lived experience and facilitating authentic, mutual contact between the therapist and client.
Historical Context: Dialogical Gestalt Therapy emerged in the 1990s and 2000s, influenced by the dialogical philosophy of Martin Buber and the postmodern turn in Gestalt therapy.
Criticisms:
Some argue that the approach may be too abstract or philosophically complex for certain clients. Critics question the specific therapeutic techniques and mechanisms of change in Dialogical Gestalt Therapy.
Dynamic Attachment Re-Patterning Experience (DARe)
Founder: Diane Poole Heller
Approach: DARe is an attachment-focused approach that aims to identify and heal early attachment wounds and patterns.
Techniques:
Somatic and embodied interventions Corrective attachment experiences Imaginal dialogues with attachment figures Integration of adult attachment styles
Focus: The focus is on promoting secure attachment patterns and resolving the impact of early attachment injuries on present-day relationships and functioning.
Historical Context: DARe was developed by Diane Poole Heller in the 2000s and 2010s, integrating attachment theory, somatic experiencing, and other trauma-informed approaches.
Criticisms:
Some argue that the approach may be too focused on early childhood experiences at the expense of present-day concerns. Critics question the empirical support for specific techniques used in DARe.
Dynamic Deconstructive Psychotherapy (DDP)
Founder: Robert J. Gregory
Approach: DDP is a treatment approach for borderline personality disorder that combines elements of psychodynamic therapy, dialectical behavior therapy, and neurocognitive interventions.
Techniques:
Validation and radical acceptance Interpersonal discrimination exercises Mindfulness and self-observing capacity Processing of enactments and projective identifications
Focus: The focus is on helping clients with BPD develop a more coherent sense of self, tolerate ambiguity and negative affect, and engage in healthier interpersonal relationships.
Historical Context: DDP was developed by Robert J. Gregory in the early 2000s, drawing on his clinical work with individuals with BPD and his integrative theoretical perspective.
Criticisms:
Some argue that the approach may be too complex or integrative for certain clients or treatment settings. Critics question the unique contributions and empirical support of DDP compared to other established treatments for BPD.
Dynamic Interpersonal Therapy (DIT)
Founders: Alessandra Lemma, Mary Target, Peter Fonagy
Approach: DIT is a brief psychodynamic therapy that focuses on the interpersonal context of depression and anxiety.
Techniques:
Identifying a central interpersonal affective focus Exploring past and present relationship patterns Encouraging affect expression and reflection Promoting interpersonal change and adaptive coping
Focus: The focus is on understanding and modifying the interpersonal patterns and emotional processes that contribute to the client’s symptoms of depression or anxiety.
Historical Context: DIT was developed in the 2000s and 2010s by researchers at the Anna Freud Centre in London, drawing on attachment theory, mentalization, and object relations theory.
Criticisms:
Some argue that the approach may be too narrowly focused on interpersonal factors at the expense of other contributors to depression and anxiety. Critics question the effectiveness of DIT compared to other brief psychodynamic therapies or established treatments for depression and anxiety.
Dyadic Developmental Psychotherapy (DDP)
Founder: Daniel Hughes
Approach: DDP is an attachment-focused therapy for children who have experienced trauma and attachment disruptions, emphasizing the importance of the caregiver-child relationship.
Techniques:
PACE (playfulness, acceptance, curiosity, empathy) Affective-reflective dialogue Narrative work and storytelling Caregiver coaching and support
Focus: The focus is on fostering secure attachment patterns, emotional regulation skills, and coherent autobiographical narratives in children with histories of trauma and attachment problems.
Historical Context: DDP was developed by Daniel Hughes in the 1990s and 2000s, integrating attachment theory, developmental psychology, and trauma-informed care.
Criticisms:
Some argue that the approach may be too intensive or demanding for certain caregivers or family systems. Critics question the empirical support for DDP compared to other established treatments for child trauma and attachment issues.
Eco-Psychotherapy
Key Figures: Theodore Roszak, Mary-Jayne Rust
Approach: Eco-Psychotherapy is an approach that integrates ecological and psychological perspectives to address the relationship between human well-being and the natural world.
Techniques:
Nature-based practices and rituals Exploration of ecological identity and values Mindfulness and sensory awareness in nature Addressing eco-anxiety and grief
Focus: The focus is on healing the human-nature relationship and promoting psychological and ecological well-being.
Historical Context: Eco-Psychotherapy emerged in the 1990s and 2000s, influenced by the fields of ecopsychology, deep ecology, and environmental psychology.
Criticisms:
Some argue that the approach may be too abstract or philosophical for certain clients or settings. Critics question the specific therapeutic mechanisms and empirical support for nature-based interventions.
Ecosystemic Structural Family Therapy (ESFT)
Founders: Celia Falicov, Jose Szapocznik
Approach: ESFT is a culturally sensitive, integrative approach to family therapy that considers the family’s broader social and cultural context.
Techniques:
Structural interventions (boundaries, hierarchy, alignments) Ecosystemic exploration of family-context interactions Cultural frame switching and bridging Multidimensional engagement strategies
Focus: The focus is on promoting adaptive family functioning and cultural resilience by addressing the interactions between family dynamics and larger social systems.
Historical Context: ESFT was developed in the 1980s and 1990s by Celia Falicov and Jose Szapocznik, integrating structural family therapy with ecological and cultural perspectives.
Criticisms:
Some argue that the approach may be too complex or integrative for certain families or treatment settings. Critics question the specific mechanisms of change and empirical support for the ecosystemic interventions in ESFT.
Elemental Psychotherapy
Founder: Walt Pierpoint
Approach: Elemental Psychotherapy is a holistic approach that draws on the symbolism and qualities of the four classic elements – earth, water, air, and fire – to promote transformative change and personal growth.
Techniques:
Exploration of personal associations with each element Use of elemental symbols and metaphors Embodiment and expression of elemental energies Integration of elemental qualities into daily life
Focus: The focus is on accessing the transformative powers of the elements within oneself to promote healing, self-discovery, and personal evolution.
Historical Context: Elemental Psychotherapy was developed by Walt Pierpoint in the 1990s and 2000s, drawing on Jungian psychology, depth psychology, and various spiritual traditions.
Criticisms:
Some argue that the approach may be too abstract or metaphorical for certain clients or presenting issues. Critics question the cultural universality and empirical support for the psychological significance of the four elements.
Embodied Relational Therapy (ERT)
Founders: Kate White, David Feinstein
Approach: ERT is a body-centered approach that integrates somatic psychology, relational psychotherapy, and mindfulness practices to address developmental trauma and attachment issues.
Techniques:
Tracking somatic experience and patterns Mindful body awareness Relational embodiment exercises Processing of traumatic memories and attachment ruptures
Focus: The focus is on promoting embodied self-awareness, self-regulation, and relational capacities to heal the effects of early developmental trauma.
Historical Context: ERT was developed by Kate White and David Feinstein in the 2000s and 2010s, building on their respective backgrounds in dance/movement therapy and energy psychology.
Criticisms:
Some argue that the approach may be too body-focused or experiential for certain clients or presenting issues. Critics question the integration of diverse somatic and relational approaches and the empirical support for ERT.
Emotional Schema Therapy (EST)
Founder: Robert Leahy
Approach: EST is an integrative approach that focuses on identifying and modifying maladaptive emotional schemas – beliefs, interpretations, and coping strategies related to emotions.
Techniques:
Emotional schema questionnaire and assessment Cognitive restructuring of emotion-related beliefs Experiential techniques for emotional processing Behavioral experiments and skills training
Focus: The focus is on helping clients develop more adaptive and flexible ways of understanding, experiencing, and responding to their emotions.
Historical Context: EST was developed by Robert Leahy in the 2000s and 2010s, integrating cognitive-behavioral, emotion-focused, and experiential approaches.
Criticisms:
Some argue that the approach may be too focused on cognitive and behavioral aspects of emotion at the expense of deeper emotional processing. Critics question the unique contributions and empirical support of EST compared to other emotion-focused therapies.
Emotion-Focused Family Therapy (EFFT)
Founders: Leslie Greenberg, Joanne Goldman, Lynne Angus, David Paivio
Approach: EFFT is an adaptation of Emotion-Focused Therapy (EFT) that focuses on helping families resolve emotional injuries, repair attachment bonds, and foster more adaptive patterns of interaction.
Techniques:
Accessing and expressing primary emotions Facilitating empathic responses and validation Promoting self-soothing and emotional regulation Repairing attachment injuries and ruptures
Focus: The focus is on promoting emotional healing, attachment security, and adaptive family functioning by transforming maladaptive emotional patterns and interactions.
Historical Context: EFFT was developed in the 2000s and 2010s by researchers and clinicians trained in EFT, seeking to apply emotion-focused principles to family therapy.
Criticisms:
Some argue that the approach may be too emotion-focused at the expense of other important family dynamics or presenting issues. Critics question the effectiveness of EFFT compared to other established family therapy approaches.
Enhanced Cognitive Behavioral Therapy (CBT-E)
Founders: Christopher Fairburn, Zafra Cooper
Approach: CBT-E is a transdiagnostic treatment approach for eating disorders that addresses the core cognitive and behavioral processes maintaining the disorders.
Techniques:
Collaborative case formulation Monitoring and regularizing eating patterns Addressing over-evaluation of shape and weight Cognitive restructuring and behavioral experiments Relapse prevention
Focus: The focus is on modifying the core psychopathology of eating disorders, rather than the specific symptoms of each disorder.
Historical Context: CBT-E was developed in the 2000s and 2010s by Christopher Fairburn and colleagues, building on their earlier work on cognitive-behavioral therapy for bulimia nervosa.
Criticisms:
Some argue that the approach may not adequately address the interpersonal and emotional factors contributing to eating disorders. Critics question the effectiveness of CBT-E for more severe or long-standing eating disorders.
Executive Function Problem Solving Treatment (EF-PST)
Founder: Mary V. Solanto
Approach: EF-PST is a cognitive-behavioral treatment for adult attention deficit hyperactivity disorder (ADHD) that focuses on improving executive functioning skills.
Techniques:
Problem-solving training Time management and organization strategies Cognitive modification of negative beliefs Behavioral activation and task initiation
Focus: The focus is on helping adults with ADHD develop practical skills and strategies to manage their symptoms and improve their daily functioning.
Historical Context: EF-PST was developed by Mary V. Solanto in the 2000s and 2010s, drawing on her research on the cognitive and behavioral aspects of ADHD in adults.
Criticisms:
Some argue that the approach may not adequately address the emotional and interpersonal impacts of ADHD. Critics question the long-term effectiveness and generalization of the skills learned in EF-PST.
Eye Movement Techniques in Psychotherapy
Key Figures: Francine Shapiro, David Grand
Approach: Eye Movement Techniques refer to a range of therapeutic interventions that use bilateral eye movements or other forms of bilateral stimulation to facilitate emotional processing and integration.
Techniques:
Eye Movement Desensitization and Reprocessing (EMDR) Brainspotting Neuro-Linguistic Programming (NLP) eye movement techniques Eye movement integration (EMI)
Focus: The focus is on using eye movements or bilateral stimulation to access and process the neurological and somatic components of traumatic memories, emotional distress, and maladaptive patterns.
Historical Context: Eye Movement Techniques gained popularity in the 1990s and 2000s, with EMDR being the most widely recognized and researched approach.
Criticisms:
Some argue that the theoretical mechanisms underlying eye movement techniques are not well-established or empirically supported. Critics question whether eye movements or bilateral stimulation are necessary components of these therapies, as opposed to other common factors.
Feminist Integrative Psychotherapy
Founder: Mary C. Agee
Approach: Feminist Integrative Psychotherapy is an approach that integrates feminist principles with various psychotherapy theories and techniques to address the unique experiences and needs of diverse women.
Techniques:
Analysis of power dynamics and social oppression Exploration of gender role socialization and identity Empowerment and assertiveness training Integration of multicultural and social justice perspectives
Focus: The focus is on promoting personal and social transformation by addressing the psychological impacts of gender-based oppression and empowering women to live authentic, self-determined lives.
Historical Context: Feminist Integrative Psychotherapy emerged in the 1990s and 2000s, building on the earlier work of feminist therapy pioneers and incorporating insights from multicultural and social justice perspectives.
Criticisms:
Some argue that the approach may overemphasize gender at the expense of other aspects of identity and experience. Critics question the integration of diverse theoretical perspectives and the specific mechanisms of change in Feminist Integrative Psychotherapy.
Glossary of Psychotherapy Terms
Abreaction: The release of emotional tension through recalling a repressed traumatic experience. (Associated with psychoanalysis)
Acceptance and Commitment Therapy (ACT): A form of therapy that uses acceptance and mindfulness strategies, along with commitment and behavior change strategies.
Affect: The observable expression of emotion.
Ambivalence: The simultaneous experience of contradictory feelings toward a person or thing.
Analytical Psychology: A form of depth psychology developed by Carl Jung. (Associated with Jungian analysis)
Anima/Animus: In Jungian psychology, the unconscious feminine side of a man (anima) or masculine side of a woman (animus). (Associated with Jungian analysis)
Anxiety: A feeling of worry, nervousness, or unease about something with an uncertain outcome.
Archetype: Universal, innate models of people, behaviors, or personalities. (Associated with Jungian analysis)
Association: The process of connecting ideas, memories, and feelings.
Attachment: The emotional bond between an infant and their primary caregiver. (Associated with attachment theory)
Automatic Thoughts: Spontaneous, often negative thoughts that occur rapidly in response to a situation. (Associated with cognitive-behavioral therapy)
Behaviorism: A psychological approach that emphasizes observable behaviors rather than internal mental states.
Biofeedback: A technique that trains people to improve their health by controlling certain bodily processes.
Catharsis: The process of releasing strong or repressed emotions.
Cognitive Behavioral Therapy (CBT): A type of psychotherapy that helps patients understand the thoughts and feelings that influence behaviors.
Cognitive Distortion: Inaccurate or exaggerated thought patterns that reinforce negative emotions. (Associated with cognitive-behavioral therapy)
Collective Unconscious: In Jungian psychology, a part of the unconscious mind shared by a society or all humanity. (Associated with Jungian analysis)
Complex: A core pattern of emotions, memories, perceptions, and wishes in the personal unconscious. (Associated with psychoanalysis and Jungian analysis)
Conditioning: The process of learning to associate a particular stimulus with a particular response. (Associated with behaviorism)
Conscious: The part of the mind that is aware of immediate thoughts, feelings, and perceptions.
Countertransference: The therapist’s emotional reaction to the patient, often based on the therapist’s own unconscious needs. (Associated with psychoanalysis)
Defense Mechanism: Unconscious psychological strategies used to cope with reality and maintain self-image. (Associated with psychoanalysis)
Dialectical Behavior Therapy (DBT): A type of cognitive-behavioral therapy that emphasizes the psychosocial aspects of treatment.
Dissociation: A psychological experience in which a person feels disconnected from their thoughts, feelings, memories, or sense of identity.
Ego: In Freudian psychology, the part of the personality that mediates between the id and the superego. (Associated with psychoanalysis)
Ego Psychology: A school of psychoanalysis that emphasizes the importance of the ego in managing psychic conflict. (Associated with psychoanalysis)
Electroconvulsive Therapy (ECT): A procedure in which electric currents are passed through the brain to trigger a brief seizure, used to treat certain mental health conditions.
Empathy: The ability to understand and share the feelings of another.
Existential Therapy: A form of psychotherapy that emphasizes the human condition as a whole, particularly themes of free will, self-determination, and the search for meaning.
Exposure Therapy: A technique in which a person is gradually exposed to an anxiety-producing object or situation. (Associated with behavioral therapy)
Family Systems Therapy: An approach that treats the family as a whole rather than focusing on individual members.
Free Association: A technique in psychoanalysis in which a person says whatever comes into their mind without censorship. (Associated with psychoanalysis)
Gestalt Therapy: A form of psychotherapy that emphasizes personal responsibility and focuses on the individual’s experience in the present moment.
Group Therapy: A form of psychotherapy that involves one or more therapists working with several people at the same time.
Humanistic Therapy: An approach that emphasizes a person’s inherent drive towards self-actualization and creativity.
Hypnosis: An altered state of consciousness characterized by heightened suggestibility and focused attention.
Id: In Freudian psychology, the part of the personality that contains unconscious psychic energy. (Associated with psychoanalysis)
Individuation: In Jungian psychology, the process of integrating the conscious with the unconscious. (Associated with Jungian analysis)
Insight: The capacity to gain an accurate and deep understanding of someone or something.
Interpretation: In psychotherapy, the therapist’s explanation of the client’s thoughts, feelings, or behaviors.
Intrapsychic: Occurring within the mind or psyche.
Libido: In Freudian theory, psychic and emotional energy associated with instinctual biological drives. (Associated with psychoanalysis)
Mindfulness: A mental state achieved by focusing one’s awareness on the present moment. (Associated with mindfulness-based therapies)
Mirroring: A therapeutic technique where the therapist reflects the client’s body language, emotions, or words.
Narcissism: Excessive interest in or admiration of oneself.
Narrative Therapy: A form of psychotherapy that separates the person from the problem and encourages them to rely on their own skills to minimize problems in their life.
Neurotransmitter: A chemical messenger that transmits signals across a synapse from one neuron to another.
Object Relations Theory: A psychodynamic theory that suggests that the way people relate to others and situations in their adult lives is shaped by family experiences during infancy. (Associated with psychoanalysis)
Oedipus Complex: In Freudian theory, a child’s unconscious desire for the opposite-sex parent, coupled with rivalry with the same-sex parent. (Associated with psychoanalysis)
Operant Conditioning: A learning process in which behavior is modified by its consequences. (Associated with behaviorism)
Persona: In Jungian psychology, the social face an individual presents to the world. (Associated with Jungian analysis)
Phenomenology: The study of structures of consciousness as experienced from the first-person point of view.
Positive Psychology: A branch of psychology that focuses on the character strengths and behaviors that allow individuals to build a life of meaning and purpose.
Preconscious: In psychoanalytic theory, the part of the mind containing thoughts and feelings that are not currently conscious but can be readily recalled.
Projection: A defense mechanism in which a person attributes their own unacceptable urges to another person. (Associated with psychoanalysis)
Psychoanalysis: A set of psychological theories and therapeutic techniques that aim to treat mental disorders by investigating the interaction of conscious and unconscious elements in the mind.
Psychodynamic Therapy: A form of depth psychology that emphasizes the study of the psychological forces underlying human behavior, feelings, and emotions.
Psychosis: A severe mental disorder in which thoughts and emotions are so impaired that contact is lost with external reality.
Rational Emotive Behavior Therapy (REBT): A form of cognitive therapy that focuses on resolving emotional and behavioral problems.
Regression: A defense mechanism in which a person reverts to an earlier stage of development. (Associated with psychoanalysis)
Reinforcement: The process of encouraging or establishing a belief or pattern of behavior. (Associated with behaviorism)
Repression: The unconscious blocking of unpleasant emotions, impulses, memories, and thoughts. (Associated with psychoanalysis)
Resistance: In psychotherapy, the client’s opposition to confronting difficult feelings or situations.
Schema: A cognitive framework or concept that helps organize and interpret information. (Associated with cognitive therapy)
Self-Actualization: The realization or fulfillment of one’s talents and potentialities. (Associated with humanistic psychology)
Shadow: In Jungian psychology, the unconscious aspect of personality which the conscious ego does not identify in itself. (Associated with Jungian analysis)
Solution-Focused Brief Therapy: A goal-directed collaborative approach to psychotherapeutic change that emphasizes finding solutions rather than focusing on problems.
Somatic Experiencing: A form of trauma therapy that focuses on perceived body sensations.
Stimulus: Any object or event that is sensed by a living organism and elicits a response.
Sublimation: A mature type of defense mechanism where socially unacceptable impulses are transformed into socially acceptable actions. (Associated with psychoanalysis)
Superego: In Freudian theory, the part of the personality that represents internalized ideals and moral standards. (Associated with psychoanalysis)
Suppression: The conscious process of pushing unwanted thoughts into the unconscious.
Systematic Desensitization: A type of behavior therapy used to treat phobias and other anxiety disorders. (Associated with behavioral therapy)
Therapeutic Alliance: The working relationship between a therapist and client.
Transactional Analysis: A psychoanalytic theory of psychology that examines a person’s relationships and interactions.
Transference: The redirection of feelings and desires, especially those unconsciously retained from childhood, toward a new object. (Associated with psychoanalysis)
Trauma: A deeply distressing or disturbing experience.
Unconditional Positive Regard: A concept developed by Carl Rogers that refers to the basic acceptance and support of a person regardless of what they say or do. (Associated with person-centered therapy)
Unconscious: The part of the mind that is inaccessible to the conscious mind but affects behavior and emotions.
Validation: The recognition and acceptance of another person’s thoughts, feelings, sensations, and behaviors as understandable.
Cognitive Restructuring: The therapeutic process of identifying and challenging negative or irrational thoughts. (Associated with cognitive-behavioral therapy)
Flooding: A type of exposure therapy where the patient is exposed to anxiety-producing stimuli intensely and rapidly. (Associated with behavioral therapy)
Genogram: A pictorial display of a person’s family relationships and medical history used in family therapy.
Inner Child: A concept used in various forms of therapy that refers to the childlike aspect of a person’s psyche.
Motivational Interviewing: A counseling approach designed to help people find the motivation to make positive behavior changes.
Negative Reinforcement: The removal of an unpleasant stimulus to increase the likelihood of a behavior. (Associated with behaviorism)
Paradoxical Intention: A cognitive reframing technique where the person is encouraged to engage in the feared behavior. (Associated with logotherapy)
Psychoeducation: The process of providing education and information to those seeking or receiving mental health services.
Reciprocal Inhibition: A behavioral therapy technique where a relaxation response is conditioned to occur in the presence of anxiety-producing stimuli.
Relapse Prevention: A cognitive-behavioral approach with the goal of identifying and preventing high-risk situations for relapse.
Sand Tray Therapy: A form of expressive therapy that uses a sandbox and miniature toys to create scenes reflecting a person’s inner world.
Self-Efficacy: An individual’s belief in their capacity to execute behaviors necessary to produce specific performance attainments. (Associated with cognitive-behavioral therapy)
Sensorimotor Psychotherapy: A body-centered approach that aims to treat the somatic symptoms of unresolved trauma.
Socratic Questioning: A form of disciplined questioning used in therapy to probe a client’s beliefs and assumptions. (Associated with cognitive therapy)
Structural Family Therapy: A type of family therapy that focuses on adjusting and strengthening the family system to improve the functioning of the family unit.
Supervision: The process where a more experienced therapist guides and oversees the work of a less experienced therapist.
Therapeutic Metaphor: The use of stories or figurative language in therapy to help clients understand their situations from a different perspective.
Token Economy: A system of behavior modification based on the systematic reinforcement of target behavior using “tokens” as secondary reinforcers. (Associated with behavioral therapy)
Triangulation: A manipulation tactic where one person will not communicate directly with another person, instead using a third person to relay communication. (Often addressed in family systems therapy)
Working Through: The process in psychotherapy of thoroughly exploring and dealing with issues or problems, often involving repetition and gradual progress.
Abstinence: In psychoanalysis, the analyst’s restraint from gratifying the patient’s desires or impulses.
Active Imagination: A method in Jungian psychology of assimilating unconscious contents through some form of self-expression. (Associated with Jungian analysis)
Adlerian Therapy: An approach to psychotherapy that emphasizes the individual’s strive for superiority and sense of belonging. (Associated with Individual Psychology)
Affect Regulation: The ability to modulate one’s emotional state.
Alexithymia: Difficulty in identifying and describing emotions.
Altered State of Consciousness: Any condition significantly different from a normal waking state.
Amplification: In Jungian psychology, the expansion and enrichment of dream images. (Associated with Jungian analysis)
Anal Stage: In Freudian theory, the second stage of psychosexual development. (Associated with psychoanalysis)
Anhedonia: The inability to feel pleasure in normally pleasurable activities.
Anomie: A state or condition of individuals or society characterized by a breakdown of social priorities and values.
Anthroposophical Medicine: A holistic and salutogenic approach to medicine developed by Rudolf Steiner.
Anticipatory Anxiety: Anxiety experienced in anticipation of a difficult situation.
Apperception: The process of understanding something perceived in terms of previous experience.
Archetypes: Primordial images and motifs that comprise the collective unconscious. (Associated with Jungian analysis)
Art Therapy: A form of psychotherapy that uses art media as its primary mode of expression and communication.
Assertiveness Training: A form of behavior therapy designed to help people stand up for themselves.
Attachment Styles: Patterns of behavior in relationships, typically formed in early childhood. (Associated with Attachment Theory)
Autogenic Training: A relaxation technique developed by Johannes Schultz.
Autonomy: Independence or freedom, as of the will or one’s actions.
Aversion Therapy: A form of behavior therapy designed to make the patient give up an undesirable habit by causing them to associate it with an unpleasant effect.
Behavioural Activation: A component of CBT aimed at increasing engagement in adaptive activities through scheduling and reinforcement. (Associated with cognitive-behavioral therapy)
Bibliotherapy: The use of books as therapy in the treatment of mental or psychological disorders.
Bioenergetics: A form of body psychotherapy combining physical exercises with psychotherapy. (Associated with body-oriented psychotherapy)
Bipolar Disorder: A mental health condition characterized by alternating periods of elevated mood and depression.
Body Dysmorphic Disorder: A mental disorder characterized by an obsessive preoccupation with a perceived defect in one’s physical appearance.
Borderline Personality Disorder: A mental health disorder characterized by unstable moods, behavior, and relationships.
Cathartic Method: A psychotherapeutic method of bringing repressed ideas and feelings into consciousness. (Associated with psychoanalysis)
Chair Work: A psychotherapeutic technique where clients use different chairs to represent different perspectives or parts of themselves. (Associated with Gestalt therapy)
Circumambulation: In Jungian psychology, the act of “walking around” the Self, approaching it from different sides. (Associated with Jungian analysis)
Classical Conditioning: A learning process in which a neutral stimulus becomes associated with a meaningful stimulus and acquires the capacity to elicit a similar response. (Associated with behaviorism)
Cognitive Dissonance: The mental discomfort experienced when simultaneously holding two or more conflicting beliefs, ideas, or values.
Collective Consciousness: The set of shared beliefs, ideas, and moral attitudes which operate as a unifying force within society.
Compensation: In Jungian psychology, the process by which the unconscious offsets deficiencies in the personality. (Associated with Jungian analysis)
Compulsion: An irresistible urge to behave in a certain way, especially against one’s conscious wishes.
Condensation: In dream interpretation, the process by which multiple dream thoughts are combined into a single image. (Associated with psychoanalysis)
Conformity: The act of matching attitudes, beliefs, and behaviors to group norms, politics or being like-minded.
Confrontation: A therapeutic technique where the therapist points out discrepancies in the client’s behavior or thinking.
Congruence: In person-centered therapy, the state of being genuine and authentic in the therapeutic relationship. (Associated with person-centered therapy)
Conversion Disorder: A mental condition in which a person has neurological symptoms that can’t be explained by medical evaluation.
Coping Mechanism: Any conscious or non-conscious adjustment or adaptation that decreases tension and anxiety.
Core Beliefs: Fundamental, inflexible, absolute, and generalized beliefs that people hold about themselves, others, and the world. (Associated with cognitive-behavioral therapy)
Counterconditioning: A form of conditioning in which a response to a stimulus is changed from one to another. (Associated with behaviorism)
Crisis Intervention: Emergency psychological care aimed at assisting individuals in a crisis situation to restore equilibrium to their bio-psycho-social functioning.
Cross-Cultural Psychology: The scientific study of human behavior and mental processes under diverse cultural conditions.
Decatastrophizing: A cognitive restructuring technique aimed at reducing catastrophic thinking. (Associated with cognitive-behavioral therapy)
Decompensation: The deterioration of existing defenses, leading to an exacerbation of pathological behavior.
Depersonalization: A state in which one’s thoughts and feelings seem unreal or not to belong to oneself.
Desensitization: A process of diminished emotional responsiveness to a negative or aversive stimulus after repeated exposure to it.
Developmental Psychology: The scientific study of systematic psychological changes that occur in human beings over the course of their life span.
Differential Reinforcement: Reinforcing only those responses within a response class that meet a specific criterion. (Associated with behaviorism)
Directive Therapy: Any form of therapy where the therapist directs the course of treatment and suggests what the client should do.
Displacement: A defense mechanism in which a drive or feeling is shifted to a substitute object. (Associated with psychoanalysis)
Dissociative Identity Disorder: A mental disorder characterized by the maintenance of at least two distinct and relatively enduring personality states.
Dream Analysis: The psychological interpretation of dreams. (Associated with psychoanalysis and Jungian analysis)
Dyad: A group of two people, typically involved in a social interaction.
Dysfunctional Thought Record: A tool used in cognitive-behavioral therapy to identify and challenge negative automatic thoughts. (Associated with cognitive-behavioral therapy)
Eclectic Therapy: An approach to psychotherapy that draws on multiple theoretical orientations and techniques.
Ego Boundary: The theoretical line differentiating the self from the external world.
Ego Dystonic: Aspects of a person’s thoughts, impulses, attitudes, and behaviors that are felt to be repugnant, distressing, or inconsistent with the rest of the personality.
Ego Ideal: In psychoanalytic theory, the part of the personality serving as a standard for the ego; an idealized self-image. (Associated with psychoanalysis)
Ego Integrity: In Erikson’s stages of psychosocial development, the ability to look back on one’s life with satisfaction.
Ego Syntonic: Aspects of one’s thoughts, behavior, or attitudes that are acceptable to the ego.
Enantiodromia: In Jungian psychology, the principle that anything pushed to an extreme converts into its opposite. (Associated with Jungian analysis)
Enuresis: Involuntary urination, especially by children at night.
Enmeshment: A condition in which two or more people, typically family members, are overly involved with and dependent on each other.
Eriksonian Therapy: A form of psychotherapy based on the psychosocial stages of development articulated by Erik Erikson.
Erotic Transference: In psychoanalysis, the client’s experience of feelings of love for the analyst. (Associated with psychoanalysis)
Existential Anxiety: Anxiety related to the human condition and questions of existence.
Externalization: A therapeutic technique used in narrative therapy where the problem is separated from the person.
Extinction: The weakening of a conditioned response when the conditioned stimulus occurs without the unconditioned stimulus. (Associated with behaviorism)
False Self: In object relations theory, a facade developed to cope with difficult relational experiences in childhood. (Associated with psychoanalysis)
Family Constellation: A therapeutic method that aims to reveal hidden dynamics in a family or relationship to address stressors.
Family Sculpting: A technique used in family therapy where family members physically position themselves to represent emotional relationships within the family.
Fixation: In psychoanalytic theory, a persistent focus on an earlier stage of psychosexual development. (Associated with psychoanalysis)
Flooding: A behavior therapy technique used to treat phobias by exposing the patient directly to the feared stimulus. (Associated with behavioral therapy)
Flow: In positive psychology, a mental state of complete absorption in the current experience.
Focusing: A psychotherapeutic process developed by Eugene Gendlin that involves attending to the body’s subtle signals.
Formal Operational Stage: In Piaget’s theory of cognitive development, the stage at which abstract thought emerges.
Fundamental Attribution Error: The tendency to overemphasize personality-based explanations for behaviors observed in others while underemphasizing situational explanations.
Galvanic Skin Response: A change in the electrical properties of the skin associated with the activity of sweat glands.
Generalized Anxiety Disorder: An anxiety disorder characterized by persistent, excessive, and unrealistic worry about everyday things.
Genogram: A pictorial display of a person’s family relationships and medical history. (Associated with family systems therapy)
Gestalt: A structure, configuration, or pattern of physical, biological, or psychological phenomena so integrated as to constitute a functional unit with properties not derivable from its parts in summation.
Grounding Techniques: Strategies to help a person focus on the present moment and connect with the physical environment.
Group Dynamics: The interactions, attitudes, and behaviors that occur within a social group.
Guided Imagery: A mind-body intervention in which a person is guided in imagining a relaxing scene or series of experiences.
Habituation: The diminishing of a physiological or emotional response to a frequently repeated stimulus.
Hakomi Method: A body-centered, somatic psychotherapy that uses mindfulness and the body as a route to core material.
Hallucination: A sensory experience of something that does not exist outside the mind.
Halo Effect: The tendency for an impression created in one area to influence opinion in another area.
Harm Reduction: A set of practical strategies and ideas aimed at reducing negative consequences associated with drug use.
Hierarchical Needs: Maslow’s theory that people are motivated by five basic categories of needs: physiological, safety, love, esteem, and self-actualization.
Holding Environment: In object relations theory, the supportive environment provided by the caregiver to the child. (Associated with psychoanalysis)
Homeostasis: The tendency toward a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes.
Homework: In cognitive-behavioral therapy, tasks assigned to clients to complete between sessions. (Associated with cognitive-behavioral therapy)
Hormesis: The theory that exposure to low doses of an agent that is dangerous in higher doses can be beneficial.
Humanism: A psychological perspective that emphasizes the study of the whole person and the uniqueness of each individual.
Hypervigilance: An enhanced state of sensory sensitivity accompanied by an exaggerated intensity of behaviors whose purpose is to detect activity.
Hypnotherapy: The use of hypnosis as a therapeutic technique.
Id Psychology: A variation of psychoanalytic theory that emphasizes the role of the id (instinctual drives) in personality and behavior. (Associated with psychoanalysis)
Identification: A defense mechanism by which an individual adopts the behaviors, values, or characteristics of another person or group. (Associated with psychoanalysis)
Idiographic: Relating to the study of individuals, as opposed to groups.
Implosion Therapy: A type of behavior therapy that attempts to weaken neurotic fears by exposing the person to anxiety-producing stimuli while preventing avoidance responses. (Associated with behavioral therapy)
Incongruence: In person-centered therapy, a state of disparity between the actual experience of the organism and the self-picture of the individual insofar as it represents that experience. (Associated with person-centered therapy)
Individual Psychology: Alfred Adler’s theory focusing on the drive to compensate for feelings of inferiority.
Individuation: In Jungian psychology, the process by which a person becomes a psychological individual, differentiated from others. (Associated with Jungian analysis)
Induction: The initial stage of hypnosis in which the subject becomes relaxed and susceptible to suggestion.
Inferiority Complex: A condition characterized by lack of self-esteem, confidence, and feelings of not measuring up to societal standards. (Associated with Individual Psychology)
Insecure Attachment: An attachment style characterized by anxiety, avoidance, or disorganization in relationships. (Associated with Attachment Theory)
Instinct: An innate, typically fixed pattern of behavior in animals in response to certain stimuli.
Integration: In Jungian psychology, the process of incorporating unconscious contents into consciousness. (Associated with Jungian analysis)
Introjection: The unconscious adoption of the ideas or attitudes of others. (Associated with psychoanalysis)
Introspection: The examination or observation of one’s own mental and emotional processes.
Isolation: A defense mechanism in which a thought or memory is stripped of its emotional content. (Associated with psychoanalysis)
Jungian Analysis: A form of analytical psychology developed by Carl Jung, emphasizing the importance of the individual psyche and the personal quest for wholeness. (Associated with Jungian analysis)
Kinesthesis: The sensation of movement or strain in muscles, tendons, and joints.
Kleptomania: A recurrent urge to steal, typically without regard for need or profit.
Latency Period: In Freudian theory, the stage of psychosexual development between the phallic stage and the genital stage. (Associated with psychoanalysis)
Learned Helplessness: A condition in which a person suffers from a sense of powerlessness, arising from a persistent failure to succeed.
Locus of Control: The degree to which people believe that they have control over the outcome of events in their lives.
Logotherapy: A type of existential analysis that focuses on a will to meaning as opposed to a Freudian will to pleasure or Adlerian will to power.
Mania: A state of abnormally elevated arousal, affect, and energy level.
Masochism: The tendency to derive pleasure, especially sexual gratification, from one’s own pain or humiliation.
Maturation: The process of becoming mature; a developmental process.
Melancholia: In psychoanalytic theory, a profound presentation of depression. (Associated with psychoanalysis)
Mentalization: The ability to understand the mental state of oneself and others which underlies overt behavior.
Metacognition: Awareness and understanding of one’s own thought processes.
Mindfulness-Based Cognitive Therapy (MBCT): A psychological therapy which uses techniques such as meditation to treat depression.
Modeling: A technique used in behavioral therapy in which the client learns by observing and mimicking others. (Associated with behavioral therapy)
Moral Development: The process through which children develop proper attitudes and behaviors toward other people in society, based on social and cultural norms, rules, and laws.
Munchausen Syndrome: A factitious disorder wherein those affected feign disease, illness, or psychological trauma to draw attention, sympathy, or reassurance to themselves.
Narcissistic Personality Disorder: A personality disorder characterized by a long-standing pattern of grandiosity, need for admiration, and lack of empathy.
Negative Reinforcement: The strengthening of a behavior because a negative condition is stopped or avoided as a consequence of the behavior. (Associated with behaviorism)
Neurodevelopmental Disorders: A group of disorders in which the development of the central nervous system is disturbed.
Neuroplasticity: The brain’s ability to reorganize itself by forming new neural connections throughout life.
Neurosis: A class of functional mental disorders involving chronic distress but neither delusions nor hallucinations.
Nondirective Therapy: A therapeutic approach in which the therapist refrains from giving advice, making suggestions, or providing interpretations. (Associated with person-centered therapy)
Object Constancy: The ability to maintain a positive emotional bond with others even when under stress or experiencing negative emotions.
Obsessive-Compulsive Disorder (OCD): An anxiety disorder in which people have unwanted and repeated thoughts, feelings, ideas, sensations (obsessions), and behaviors that drive them to do something over and over (compulsions).
Ontogenesis: The development or developmental history of an individual organism.
Operationalization: The process of strictly defining variables into measurable factors.
Oral Stage: In Freudian theory, the first stage of psychosexual development. (Associated with psychoanalysis)
Organic Mental Disorder: A syndrome characterized by a clinically significant decline in cognitive functions due to a medical condition not directly related to a psychiatric illness.
Panic Attack: A sudden episode of intense fear that triggers severe physical reactions when there is no real danger or apparent cause.
Paranoid Personality Disorder: A mental condition in which a person has a long-term pattern of distrust and suspicion of others without adequate reason.
Paraphrasing: A therapeutic technique in which the therapist restates the client’s words to show understanding and encourage further exploration.
Passive-Aggressive Behavior: A pattern of indirectly expressing negative feelings instead of openly addressing them.
Pedophilia: A psychiatric disorder in which an adult or older adolescent experiences a primary or exclusive sexual attraction to prepubescent children.
Perseveration: The repetition of a particular response (such as a word, phrase, or gesture) despite the absence or cessation of a stimulus.
Personality Inventory: A questionnaire designed to assess personality traits or types.
Phallic Stage: In Freudian theory, the third stage of psychosexual development. (Associated with psychoanalysis)
Phobia: An irrational and excessive fear of an object or situation.
Placebo Effect: A beneficial effect produced by a placebo drug or treatment, which cannot be attributed to
Phobia: An irrational and excessive fear of an object or situation.
Placebo Effect: A beneficial effect produced by a placebo drug or treatment, which cannot be attributed to the properties of the placebo itself.
Play Therapy: A form of therapy primarily used with children, in which play is used as a means of communication and expression.
Positive Psychology: The scientific study of the strengths that enable individuals and communities to thrive.
Post-Traumatic Stress Disorder (PTSD): A mental health condition triggered by experiencing or witnessing a terrifying event.
Practicum: Supervised clinical experience provided to graduate students in psychology and other mental health professions.
Preconscious: In psychoanalytic theory, the thoughts and feelings that are not conscious but can be brought into consciousness easily. (Associated with psychoanalysis)
Primary Process Thinking: In Freudian theory, the type of mental activity most characteristic of the unconscious. (Associated with psychoanalysis)
Projective Test: A type of personality test in which a person responds to ambiguous stimuli, revealing hidden emotions and internal conflicts.
Psychodrama: A form of psychotherapy in which clients use spontaneous dramatization, role playing, and dramatic self-presentation to investigate and gain insight into their lives.
Psychogenic: Having a psychological origin or cause rather than a physical one.
Psychomotor Agitation: A set of signs and symptoms that stem from mental tension and anxiety.
Psychoneuroimmunology: The study of the interaction between psychological processes and the nervous and immune systems of the human body.
Psychopathology: The scientific study of mental disorders, including their symptoms, etiology, and treatment.
Psychosexual Stages: In Freudian theory, the stages of development in which the id’s pleasure-seeking energies focus on different parts of the body. (Associated with psychoanalysis)
Psychosocial Development: Erikson’s theory of eight stages of human development, each characterized by a specific psychosocial crisis.
Psychosomatic: Of or relating to a physical illness or other condition caused or aggravated by a mental factor such as internal conflict or stress.
Psychosynthesis: An approach to psychology that emphasizes spiritual and transpersonal aspects of the psyche.
Purging: The act of ridding the body of food, often after binge eating, as a feature of certain eating disorders.
Rapport: A close and harmonious relationship in which the people or groups concerned understand each other’s feelings or ideas and communicate well.
Reaction Formation: A defense mechanism in which a person goes beyond denial and behaves in the opposite way to which he or she thinks or feels. (Associated with psychoanalysis)
Reality Testing: The ability to distinguish between internal experiences and the external world.
Reattribution: A cognitive technique used to identify and challenge thoughts about the cause of negative events. (Associated with cognitive-behavioral therapy)
Rebirthing: A form of breathwork that is intended to release suppressed traumatic childhood memories.
Reciprocal Inhibition: In behavior therapy, the process by which a new response incompatible with an unwanted response is conditioned to occur in the presence of the stimulus that formerly elicited the unwanted response. (Associated with behavioral therapy)
Reconsolidation: The process by which previously consolidated memories are recalled and actively consolidated again, in which they are vulnerable to change.
Regression to the Mean: The phenomenon that if a variable is extreme on its first measurement, it will tend to be closer to the average on its second measurement.
Reinforcement Schedule: In operant conditioning, the protocol for determining when and how often a behavior is reinforced. (Associated with behaviorism)
Relational Psychoanalysis: A school of psychoanalysis that emphasizes the role of real and imagined relationships with others in mental disorder and psychotherapy.
Relaxation Response: A physical state of deep rest that changes the physical and emotional responses to stress.
Repetition Compulsion: In psychoanalytic theory, the tendency to repeat traumatic or problematic experiences. (Associated with psychoanalysis)
Resilience: The ability to mentally or emotionally cope with a crisis or to return to pre-crisis status quickly.
Resistance: In psychoanalysis, the patient’s opposition to recognizing or accepting repressed material. (Associated with psychoanalysis)
Restraint: A measure or condition that keeps someone or something under control or within limits.
Retroactive Inhibition: The interfering effect of new learning on the recall of previously learned material.
Rorschach Test: A projective psychological test in which subjects’ perceptions of inkblots are recorded and then analyzed using psychological interpretation.
Sadism: The tendency to derive pleasure, especially sexual gratification, from inflicting pain, suffering, or humiliation on others.
Salutogenesis: An approach focusing on factors that support human health and well-being, rather than on factors that cause disease.
Scapegoating: The practice of singling out a person or group for unmerited blame and consequent negative treatment.
Schizoid: A personality type characterized by emotional coldness and detachment from social relationships.
Secondary Gain: The advantage or privilege a person derives from having an illness or disability.
Self-Actualization: In Maslow’s hierarchy of needs, the highest level of psychological development where personal potential is fully realized.
Self-Fulfilling Prophecy: A prediction that directly or indirectly causes itself to become true.
Self-Harm: The intentional, direct injuring of body tissue, done without suicidal intentions.
Sensitization: An increase in the strength of a response to a repeated stimulus.
Separation Anxiety: Excessive fear or anxiety about separation from home or an attachment figure.
Sequelae: A condition which is the consequence of a previous disease or injury.
Sociometry: A quantitative method for measuring social relationships developed by psychotherapist Jacob L. Moreno.




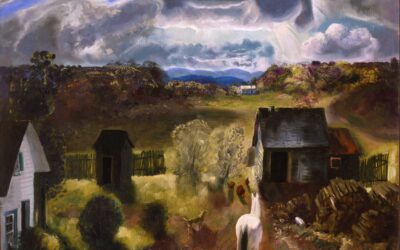













0 Comments