
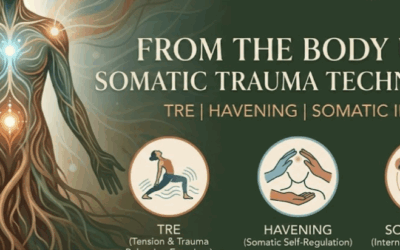
Reckoning with the Spiritual and Mystical in Neurology
Bridging the divide between empirical neuroscience and the subjective human soul.

Modern clinical psychology is currently engaged in a profound internal conflict. On one side sits the empirical demand for objective, quantifiable "behavioral" data. On the other sits the messy, unquantifiable, and profoundly subjective reality of human phenomenology. If we reduce a patient entirely to neurochemical data points, we strip them of their humanity. But if we abandon the rigors of neuroscience, we risk slipping into baseless mysticism.
At Taproot Therapy Collective, we believe that the most effective healing occurs precisely at the intersection of the objective brain and the subjective mind. To achieve true integration, we must reckon with how our ancient neurology constructs our most deeply held spiritual and relational realities.
The Polyvagal Theory and the Biology of Attachment
Dr. Stephen Porges' Polyvagal Theory has revolutionized our understanding of the autonomic nervous system's (ANS) role in regulating emotional states and social engagement (Porges, 2011). According to this framework, the ANS is not just a biological survival mechanism; it is the biological foundation of attachment and connection.
In a secure attachment scenario, where caregivers are attuned and responsive, the ventral vagal complex promotes feelings of safety. This neurological state allows for a healthy emotional arc: emotions rise, peak, and resolve in a regulated manner. The prefrontal cortex (associated with explicit memory and logic) can process and make sense of these experiences, while the subcortical regions (linked to implicit memory) store the "felt sense" of safety and resolution (Siegel, 2012).
However, in insecure or traumatic attachment styles, the autonomic nervous system becomes dysregulated due to inconsistent or threatening caregiving (Schore, 2001). In avoidant attachment, the dorsal vagal complex may become overactive, triggering a biological "shutdown." This leads to profound emotional suppression and disconnection. The individual avoids the emotional arc entirely, because the implicit memory of danger overrides the explicit memory of the actual event. The body remembers the threat, even when the logic center insists everything is fine.
Memory, Neurology, and the Fragmented Arc
When traumatic experiences disrupt neural integration, the individual becomes stuck in incomplete emotional arcs, resulting in dissociation and psychological fragmentation.
The neuroscience of memory reconsolidation suggests that our "sense of self" is not a fixed, unitary entity. Rather, it is an ongoing construction built from the synthesis of multiple memory networks (Siegel, 1999). Implicit memories (procedural and emotional) are encoded in the subcortical, primitive regions of the brain. Explicit memories (semantic and episodic narrative) are handled by the newer prefrontal cortex. For a traumatic event to be resolved, these disparate memory systems must synchronize.
The Rupture of the Self
Trauma causes a literal rupture in this integration process (van der Kolk, 2014). The individual becomes biologically stuck in a specific phase of an emotional arc—such as the rising intensity of panic or the peak of terror—unable to move toward resolution. This manifests as a paradoxical tension between different "parts" of the self. As observed in Parts-Based Therapy (IFS), some aspects of the psyche hold the traumatic memory, while other parts heavily dissociate from it to protect the ego (Bromberg, 1998).
Healing involves embracing these paradoxical tensions and allowing space for all aspects of the psyche to coexist, a concept deeply rooted in Jungian depth psychology (Jung, 1939). By acknowledging the contradictory parts of the self—the wounded and the resilient, the fearful and the courageous—the individual can bridge the dissociative gaps and move toward a flexible sense of identity.
Edinger on the Objective vs. Subjective Brain
Post-Jungian scholar Edward Edinger’s work in Ego and Archetype sheds light on the fundamental disagreement between two parts of the brain—a conflict that may be at the root of the split between implicit and cognitive memory in traumatic ANS regulation (Edinger, 1972).
Edinger posits that we have an inherently objective brain (the ego/prefrontal cortex) and an inherently subjective brain (the feeling/subcortical region) that are in constant disagreement. Trauma exacerbates the war between these two centers. True healing, therefore, represents a synthesis. The authentic self is a process, not a destination. Both the subjective and objective minds must be brought into awareness without one mastering or repressing the other.
Fascinatingly, modern evolutionary biology supports Edinger's perspective. Research indicates that the evolution of the precuneus in the brain of Homo sapiens is deeply linked to our capacity for religious and spiritual thought (Rappaport & Corbally, 2018). As consciousness evolved, ancient instinctual drives were pushed into what Carl Jung called the Collective Unconscious (Neumann, 1954). The modern anxiety described by Edinger is the literal friction between the needs of the objective prefrontal cortex and the ancient instincts of the subjective subcortical brain.
Academia, Bureaucracy, and the Defense of Psychology
The tension between the objective and the subjective is something that modern clinical models often hold poorly. Most therapeutic frameworks validate either mostly subjective experiences or mostly objective behaviors, depending on the biases of the founder. Objective models run the risk of ignoring the roots of trauma in the deep brain, while purely subjective models risk prioritizing feelings over the demands of existential reality.
Introducing more subjectivity, qualitative data, and intuitive rationale to psychotherapy is something that academia fiercely resists. It is wonderful to have an empirical basis for reality, but there are psychic spaces that objectivity simply cannot go. There is a deep insecurity among some academics that unless something is provable with a number, it isn't real.
I would counter that anything composed completely of empirical variables is not psychology. I am not arguing for pseudoscience or the impulsive application of whim disguised as intuition. I am arguing that real science is bigger than purely empirical randomized controlled trials. Soft sciences do not fit perfectly into objective measurements.
Psychology becomes corrupted when it is placed entirely in the hands of bureaucrats and accountants who reduce human suffering to billable "behavioral" codes. “Behavioral health” is a despicable reductionism employed as a cudgel to drive anyone capable out of mental healthcare. I do not practice “behavioral health.” I practice psychology.
Bibliography & References
Bromberg, P. M. (1998). Standing in the spaces: Essays on clinical process, trauma, and dissociation. Psychology Press.
Edinger, E. F. (1972). Ego and archetype. Shambhala Publications.
Jung, C. G. (1939). The integration of the personality. Farrar & Rinehart.
Neumann, E. (1954). The origins and history of consciousness. Princeton University Press.
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton & Company.
Rappaport, M. B., & Corbally, C. (2018). Evolution of religious capacity in the genus Homo: Trait complexity in action through compassion. Journal of Religion and Science, 53(1), 198-239.
Schore, A. N. (2001). The effects of early relational trauma on right brain development, affect regulation, and infant mental health. Infant Mental Health Journal, 22(1-2), 201-269.
Siegel, D. J. (2012). The developing mind: How relationships and the brain interact to shape who we are (2nd ed.). Guilford Press.
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Viking.



















0 Comments